
September 2018 School of Medicine, EUC/Student Handbook
… 1
EUC School of Medicine
Handbook & Course Catalogue
2018 – 2019

September 2018 School of Medicine, EUC/Student Handbook
… 2
Disclaimer
All information in the EUC Student Handbook & Course Catalog are subject to revision, with
changes in course offerings, academic rules and instruction plans. Information contained
herein supersedes previously published descriptions and is subject to change.

September 2018 School of Medicine, EUC/Student Handbook
… 3
Table of Contents
SECTION I: GENERAL INFORMATION ....................................................................................... 5
1. Mission and Outcomes ............................................................................................................. 6
1.1 Mission – Vision - Values .................................................................................................... 6
Medical School Organization - Administration ........................................................................... 8
Clinical Training at EUC ............................................................................................................... 9
Clinical training assistant .......................................................................................................... 11
Student Health and Safety Officer: ............................................................................................ 11
Academic Advisors .................................................................................................................... 12
Academic (Pre-Clinical) Advisors .............................................................................................. 12
Clinical Training Advisors .......................................................................................................... 13
Medical School General Policies ............................................................................................... 13
Academic Calendar .................................................................................................................... 18
Student Assessment Methods ................................................................................................... 21
Components of Clinical Training Assessment ......................................................................... 22
Remediation Policy for Absentees or Low GPA ....................................................................... 26
SECTION II: ACADEMIC & CLINICAL REQUIREMENTS FOR MD PROGRAM ........................ 26
Phase I: Foundations of Medicine (Years 1 -2) ......................................................................... 27
Structure & Function: From Molecules to Cells ........................................................................ 27
Structure & Function: Body System in Health I......................................................................... 27
Structure & Function: Body System in Health II........................................................................ 28
Structure & Function: Body System in Health III ....................................................................... 28
Medical Student Competencies ................................................................................................. 31
Self-Directed Learning – Computer Assisted Learning ........................................................... 35
SECTION III: STUDENT RESOURCES ...................................................................................... 36
Library ...................................................................................................................................... 36
Moodle ...................................................................................................................................... 36
USMLE Services ....................................................................................................................... 37
SECTION IV: STUDENT HEALTH & SERVICES ........................................................................ 39
Health Requirements .................................................................................................................. 39
Student Health and Safety ......................................................................................................... 40

September 2018 School of Medicine, EUC/Student Handbook
… 4
Counseling and Mental Health Support .................................................................................... 41
SECTION V: COURSE CATALOG & DESCRIPTIONS .............................................................. 42
Foundations in Medicine Year 1 ................................................................................................ 42
Foundations in Medicine Year 2 ................................................................................................ 47
Foundations of Clinical Practice Year 3 .................................................................................... 52
Clinical Medicine Core Year 4 ................................................................................................... 57
Clinical Medicine Core Year 5 ................................................................................................... 59
Clinical Medicine Core Year 6 ................................................................................................... 61
Elective Courses (Pre-Clinical and Clinical) .............................................................................. 63

September 2018 School of Medicine, EUC/Student Handbook
… 5
Section I: General Information
Welcome Message
On behalf of the European University Cyprus School of Medicine faculty, clinical teaching personnel,
staff and administration, welcome to the Clinical Training Core Program. Our exceptional and
diverse faculty and personnel are fully committed to the dissemination of medical knowledge and
the training of a new generation of competent physicians. We are dedicated to the teaching process
as we constantly aim to improve and embrace modern principles of medical education. At EUC, we
continuously strive towards providing an optimal learning environment by: 1) constantly improving
our understanding of medical knowledge; 2) remaining innovative, both in our curriculum and
teaching practices; and 3) inspiring our student to be passionate about providing their patients with
the best possible care.
Medical Education at EUC embraces a spiral, competency-based curriculum designed to introduce
students to the best practices in patient care, using innovative teaching strategies, exposure to
advanced simulation training, and much more. The horizontally integrated, spiral program of the
first three years of the Structure – Function curriculum, where students learn clinical skills from their
first year, was designed to ensure a smooth transition from basic to clinical science applications.
As we enter the Era of Bioinformatics, medical educators are challenged to seek innovative teaching
methods that address the multitude and magnitude of scientific, technological and demographic
factors that have converged to revolutionize today’s approach to human health and well-being.
These advancements not only bring challenges and new demands to today’s physicians, but also to
today’s medical educators. EUC’s mission is to prepare our students to excel in the art of healing,
but also to become inspired innovators for the advancement of knowledge and patient-centered
healthcare.
Our affiliation with state-of the art clinics and hospitals affords our students with a unique clinical
learning experience. Each center is a foremost healthcare provider. With this exposure to an
incredible diversity of patients, our graduates emerge fully prepared to practice medicine in this
increasingly global society. Our aim is that our students experience a full spectrum of health care
environments.
EUC is stepping to the forefront of global medical and health education. We are dedicated to
preparing the healthcare leaders of tomorrow, with outstanding clinicians and scientists who will
contribute to the advancement of science and medicine across the globe.
Professor G. Petrikkos Professor E. Johnson
Dean Vice Dean

September 2018 School of Medicine, EUC/Student Handbook
… 6
1. Mission and Outcomes
1.1 Mission – Vision - Values
The Mission of the School of Medicine is to educate medical students, graduate students,
and postdoctoral fellows in accordance with the highest professional standards; to train
competent and caring physicians to practice patient-centered medicine of the highest
standard; and to identify and answer fundamental questions in the mechanisms, prevention
and treatment of disease, in health care delivery and in the basic biomedical sciences.
The Vision of the undergraduate curriculum is to produce leaders in Medicine who will learn
to apply the foundation of a broad medical education to improve health at a National and
International level through patient care, research, and education.
The core Values of the EUC School of Medicine are
Excellence in the conduct of education, research, patient care and community
engagement
Integrity Acting with honesty, accountability & social responsibility
Respect Demonstrated by civility and communication worthy of the trust
given to us as teachers, scholars and healers
Collaboration Fostering creative partnerships with open communication
Community Dedication to improve the quality of life of the community
Transparency Promoting an atmosphere of openness to promote quality in
medical education, research and clinical care
Educational Strategy
The six-year curriculum at European University Cyprus is fully integrated both horizontally
(systems-based) and vertically (spiral-design) and is divided in three educational phases.
Phase I: Foundations of Medicine (years 1-2)
Phase II: Foundations of Clinical Practice (year 3)
Phase III: Clinical Medicine Core (years 4-6)
The curriculum at EUC engages multiple active and cooperative learning strategies.
Innovated and web-based educational resources have been tightly intercalated in the
program. The underlying educational aim underpinning the EUC Medical Curriculum is

September 2018 School of Medicine, EUC/Student Handbook
… 7
constructivism, which allows students to learn and create their own constructs of medical
knowledge.
General Competencies
The EUC School of Medicine curriculum has been designed to facilitate the development of
important competencies in our students. As a measure of his or her competence, every
EUC Medical School graduate will:
Apply scientific principles and a multidisciplinary body of scientific knowledge to the
diagnosis, management, and prevention of clinical problems.
Understand the variation in the expression of health and disease through critical
evaluation of biomedical research.
Obtain a sufficient level of medical knowledge to understand the basic facts,
concepts, and principles essential to competent medical practice at a local and global
level.
Exhibit the highest level of effective and efficient performance in data gathering,
organization, interpretation and clinical decision making in the prevention, diagnosis,
and management of disease.
Understand and respond to factors that influence the social, behavioral, and
economical factors in health, disease and medical care.
Demonstrate effective and compassionate interpersonal communication skill toward
patients and families necessary to form and sustain effective medical care.
Present information and ideas in an organized and clear manner to educate or inform
patients, families, colleagues and community.
Display the personal attributes of compassion, honesty and integrity in relationship
with patients, families, and the medical community.
Adhere to the highest ethical standards of judgment and conduct as it applies to the
health care milieu.
Demonstrate a critical self-appraisal in his/her knowledge and practice of medicine,
as well as received and give constructive appraisal to/from patients, families,
colleagues and other healthcare professionals.
Understand the limits of personal knowledge and experience and will demonstrate
the intellectual curiosity to actively pursue the acquisition of new knowledge and skills
necessary to refine and improve his/her medical practice or to contribute to the
scientific body of medical knowledge.
Conduct innovative and collaborative research (with behavioral and social
sciences) and integrate this knowledge into the practice of medicine.

September 2018 School of Medicine, EUC/Student Handbook
… 8
Medical School Organization - Administration
Dean
Chair
Clinical Training
Committee
S&F
Coordinator
& Committee
Chair Division
Internal
Medicine
Chair Division
Surgery
air Division
Surgery
Chair Division
Child / Maternal
Health
Chair Division
Neurosci/Mental
Health &
Sensory
Hospital Coordinator
Clinical Ed (HCCE)
Affiliated Hospital
Dept Clerkship
Coordinator (DCC)
Internal Medicine
DCC
Surgery
DCC
Child /
Maternal
Health
DCC
Neurosci/Menta
l Health &
Sensory
Chair Division
Functional Sciences
Chair Division
Structural Sciences
Course
Heads
Course
Heads
Course
Coordinator
Course
Coordinator
Course
Coordinator
Course
Coordinator
Clinical Instructors
Curriculum
Committee
Strategy & Institutional
Advisor
Ch Division
Social Med/
Public Health/
Primary Care
DCC
Social
Med/Public
Health/
Primary Care
Course
Coordinator
Vice Dean
Vice Chair

September 2018 School of Medicine, EUC/Student Handbook
… 9
Clinical Training at EUC
EUC has a formal administrative and academic structure for facilitating the clinical training
of its medical students at its affiliated hospitals. The Dean, in collaboration with the Deputy
Dean and Chair, oversees and is responsible for the Clinical Training (Clerkship) programs
at EUC, School of Medicine. As such, they are not members of any clinical training
committee. The School council appoints a seven-member Clinical Training Committee
(CTC), who are all full-time faculty and Chairs of the Clinical Divisions (see below) and the
committee elects by majority a Chairman. (When available, senior faculty members are
selected as Chairs of the Clinical Divisions and the Chairman of the CTC). The Chairs
appoint by majority vote, two additional full-time faculty members (any rank). The Office of
the Dean can include additional full- or part-time faculty in the CTC, under special
circumstances.
The Clinical Training Committee:
Oversees the planning of clinical training for all years of study
Assists the Dean in recruiting and assigning academic and clinical faculty in clinical
training
Are the liaison between the clinical training sites and the faculty responsible for
academic program and course content (Hospital coordinators and Course
Coordinators)
Ensures optimal cooperation between all affiliated persons and sites
Ensure appropriate training of scientific (clinical) collaborators and clinical instructors
Ensures optimal function of clinical training courses across all years of study
Ensures an environment of safe collaboration between the School and affiliated
healthcare sites
Assists the Dean in administrative, financial and other relevant obligations of the
School of Medicine related to the clinical training
Ensures that the learning objectives outlined for clinical training are achieved
Ensures accurate, complete and objective student evaluation
Works in collaboration with the academic and hospital coordinators, to solve any
issues that may arise up during clinical training
Oversees appropriate completion and evaluation of the logbooks
The medical program at EUC is comprised of 7 primary Divisions (5 of which are Clinical
Divisions), to which the courses and subjects are distributed. The Chairs of the Clinical
Divisions (Internal Medicine, Surgery, Child & Maternal Health, Social Medicine/Public
health/Primary Care, and Neuroscience/Mental Health/Sensory Systems) are full-time
senior faculty (Associate Professor or Professor) and are responsible for the overall
academic content and coordination of the courses taught in that Division. They oversee
clinical program and rotations at each affiliated hospital and ensure equality of training for
EUC students across all clinical training sites.
The Division Chairs work with heads of each course (Course Coordinators) taught in that
Division, who are also full-time faculty and coordinate the instruction of the course by full-
time faculty and scientific / clinical collaborators (part-time teaching faculty). Clinical
Collaborators are healthcare professionals who hold a medical specialization and a
doctoral degree, as defined by the EUC Charter. Posts of Scientific (Clinical) Collaborators
are contractual for the duration of one or two academic semesters, which may be renewed.
The Council of School of Medicine identifies the needs for positions, which are confirmed
September 2018 School of Medicine, EUC/Student Handbook
… 10
by the Dean in consultation with the Vice-Rector of Academic Affairs and the Department
of Human Resources. A Committee consisting of Departmental Faculty members assesses
the scientific qualifications and experience of each candidate for each specific
position/discipline and prepares a detailed report with supporting documentation. Based on
the Committee’s report, the final selection is made by the School Council.
Administration
Dean, School of Medicine
Prof. George Petrikkos
Deputy Dean, School of Medicine
Prof. Elizabeth O. Johnson
Chair, School of Medicine
Prof. Ioannis Patrikios
Vice Chair, School of Medicine
Prof. Theodoros Xanthos
Strategy & Institutional Advisor
Advisor of Clinical Studies & Hospital Affiliations
Prof. Vasilios Zerris
Clinical Divisions: Chairs & Chair Assistants
Internal Medicine
Chair: Constantinos Tsioutis, Lecturer
Chair Assistant: Aris Angouridis, Lecturer
Surgery
Chair: Ingeborg Friehs, Associate Prof.
Chair Assistant: Dimitrios Ntourakis, Lecturer
Child & Maternal Health
Chair: Theoklis Zaoutis, Prof.
Chair Assistant: Pantelis Trompoukis, Asst. Prof.
Neuroscience, Mental Health & Sensory Systems
Chair: Gerhard Friehs, Prof.
Chair Assistant: George Hadjigeorgiou, Lecturer
Social Medicine (Public Health & Primary Care)
Chair: Anastasia Symeou, Special Scientist
Chair Assistant: Eirini Agapidaki, Lecturer
Contact Information
Questions can be addressed to:
Eva Charalambous, Administrator

September 2018 School of Medicine, EUC/Student Handbook
… 11
Clinical Training Committee (CTC):
The Committee is comprised ex officio by the 5 Chairs / Directors of the Clinical Divisions.
The Chairs appoint by majority vote, two additional full-time faculty members (any rank).
The CTC reports to the Office of the Dean.
The Chair of the Committee (Associate or Full Professor) is determined by majority vote by
the entire Committee.
1. Constantinos Tsioutis, Lecturer
2. Ingeborg Friehs, Associate Professor
3. Theoklis Zaoutis, Professor
4. Gehardt Friehs, Professor
5. Anastasia Symeou, Special Scientist
6. Pantelis Trompoukis, Assistant Professor
7. Nikos Karpettas, Lecturer
Clinical training assistant
A clinical training assistant is appointed to assist the CTC in various matters regarding
clinical training coordination, including clinical training schedule preparation,
communication with external parties (including hospitals, clinical instructors and the Ministry
of Health), student vaccination forms, compensation of affiliated clinical sites and clinical
instructors, on-site supervision of student attendance, etc.
Clinical training Assistant: Mr. Charalambos Pittas
Student Health and Safety Officer
An Occupational medicine specialist, a General Physician or an Internist is appointed to
oversee health requirements and vaccinations of all students and keep record of any health
issues that might arise (eg.acute conditions that affect student attendance or performance).
It is clear that the Student Health and Safety Officer is not responsible for management of
any acute or chronic health conditions of the students of EUC.
Student Health & Safety Officer: Dr. Constantinos Tsioutis
Assistant Health & Safety Officer: Dr. Aris Angouridis
Nurse Assistant: Mr. Charalambos Pittas

September 2018 School of Medicine, EUC/Student Handbook
… 12
Academic Advisors
Counseling Center
Students in need of personal counseling should contact the Office of Student Affairs to
arrange a confidential, one-on-one meeting with a qualified professional. The service is also
available to academic and administrative personnel to help individuals cope with any
emotional and psychological challenges. A counselor is available on campus for
consultation by appointment throughout the academic year.
Student Advisors
The Advisors are full-time employees of the Student Advising Center, which assigns
students to individual Advisors. A first meeting is arranged to discuss the student’s interests
and career objectives, and to decide on course options. A Registration Form is then
completed and signed by both parties, to be submitted to the Office of the Registrar.
Students are encouraged to contact their Advisor at any time during the academic year.
However, it is mandatory to meet at least once a semester to discuss course options.
Meetings may be arranged during office hours or by appointment. The Student Advising
Center is located at the ground floor of the West Block building.
Academic (Pre-Clinical) Advisors
Each student is also assigned an Academic Advisor, to track each individual student from
year 1 through year 3 (semesters 1 – 6). Academic Advisors are full-time faculty of the
School of Medicine, and are responsible for assisting the student in defining and
developing realistic educational goals, in keeping with his/her abilities, skills, interests, and
career aspirations. Academic Advisors are also responsible for ensuring the student is
aware of university regulations and policies.
Academic Advisor Assignments (Pre-Clinical Years):
Class 2018/2024
Eirini Agapidaki
A - D
Constantinos Michaelides
E - I
Ilias Nikas
J - M
Dimitrios Ntourakis
N - P
Ioannis Patrikios
Q - S
Anastasis Stephanou
T - V
Theodoros Xanthos
W - Z
Class 2017/2023
A. Stephanou Section B
I. Patrikios Section A
Class 2016/2022
D. Ntourakis
I. Nikas

September 2018 School of Medicine, EUC/Student Handbook
… 13
Clinical Training Advisors
The Clinical Training Committee assigns full-time faculty members to serve as Clinical
Training Advisors to track each individual clinical student from year 4 through year 6
(semesters 7 – 12). Each advisor ensures that all requirements are correct and complete,
including: reviewing evaluation, grades and graduation requirements and updating rotation
schedules. Students must maintain contact with their Clinical Training Advisor throughout
their clinical terms until graduation.
Clinical Training Advisors
1. Full-time faculty members, clinical doctors, assigned by Clinical Training Committee
2. Each advisor ensures that all requirements are correct and complete
3. Review evaluations, grades and graduation requirements and updating rotation
schedules.
4. Students must maintain contact with their Clinical Training Advisor throughout their
clinical terms until graduation.
Clinical Training Advisor Assignments:
Class 2015/2021
Aris Angouridis
A - D
Ingeborg Friehs
E - I
Goerge Hadjigeorgiou
J - M
Nikos Karpettas
N - R
Pantelis Trompoukis
S - V
Constantinos Tsioutis
W - Z
Class 2014/2020
C. Tsioutis
Class 2013/2019
C. Tsioutis
Medical School General Policies
GENERAL POLICIES (Details can be found in the University Bulletin)
Averaging Grades
A Grade Point Average (G.P.A.) is determined for each student at the end of each semester.
The Grade Point Average (G.P.A.) is computed by multiplying the number of credit hours of
each course by the grade points equivalent to the letter grade received, and then adding
them. The sum total is then divided by the total number of credit hours for which the student
has received a grade. Grades reported as "I", "W", "P", "AU", "PE" or "GP" are not computed
in the average.
COURSES ON A PASS/FAIL BASIS
Undergraduate students in good academic standing may choose up to 12 semester hours
of credit towards a degree to be graded on a pass-fail basis. A student may be allowed to

September 2018 School of Medicine, EUC/Student Handbook
… 14
take a maximum of two courses on pass/fail basis per academic year. Courses in a student's
major and those considered as correlated to his major, cannot be taken as pass/fail. Only a
grade of "F" will be computed into the G.P.A. Students must notify the Office of the Registrar
of their intention to take a pass/fail course within the first ten weeks of a Fall or Spring
semester, or the first two weeks of a summer session.
WITHDRAWAL FROM COURSES
Students receive no credit for courses they choose to withdraw from. All withdrawals are
subject to the tuition refund policy cited in the University Bulletin.
a. Withdrawal initiated by student
A student has the responsibility to officially withdraw from a course that he or she does not
intend to complete. A student must complete the official “withdrawal form” and submit it to
the Office of the Registrar. Students who withdraw from a course before the dates listed
below will receive a grade of ‘W’ that will not affect the student’s G.P.A.
Fall and Spring Semesters: End of tenth week of classes
Summer Session: End of third week of classes
Students who do not file for withdrawal with the Office of the Registrar within this time
continue to be registered for the course(s) and if they have not completed the requirements
of the course(s), will be assigned an ‘F’ as a final grade.
WITHDRAWAL FROM THE UNIVERSITY
Students wishing to withdraw from the University must file a "Withdrawal Form" at the Office
of the Registrar. It is the student's obligation to complete this final procedure. Failure to do
so leaves the student liable for all of the current semester's tuition and fees and will result
in grades of "F" being assigned automatically to the student’s courses.
REPETITION OF WORK
If a student repeats a course, the new grade will be included in the student's cumulative
grade point average. The grade previously earned will not be included in the student's
overall grade point average, although it will be listed on the student's permanent academic
record and transcript.
CHANGE OF GRADE
Once grades have been submitted to the Office of the Registrar no changes are allowed,
unless an instructor completes a "Grade Change” form, in which he/she explains that a
legitimate error has been made in the calculation of a student's grade.
APPEALS PROCEDURE
In the case where a student believes that the grade received is different from what was
expected, he/she must exhaust all possibilities of resolving the problem with the pertinent
instructor first. If this does not lead to a resolution, the student may appeal against the grade
by filing a petition with the Office of the Registrar.
The Registrar will forward a copy of the petition to the pertinent Chairperson of Department,
who will first ascertain that no error was made by the instructor, and if so will assign an
anonymous re-evaluation of the final examination/project to another instructor. In the case
of major discrepancy between the instructor’s evaluation and the re-evaluation that will
require change of grade, the average of the two evaluations will be assigned as the final

September 2018 School of Medicine, EUC/Student Handbook
… 15
grade to the final examination/project. Changes of grades resulting from an appeal require
the endorsement of the Dean of School.
For a petition to be reviewed, a student must appeal within four (4) weeks from the date the
results are announced.
PROBATION
Any student, whose cumulative G.P.A. falls below "C" or its equivalent (2.0 G.P.A.) is placed
on probation. A student who remains on probationary status for two consecutive semesters
faces possible dismissal from the University.
PROBATION RULE (approved by Senate)
The School of Medicine expects all medical students to fulfill their responsibilities and
conduct themselves in a competent, professional manner, and to follow the rules,
regulations and policies of the European University of Cyprus and affiliated hospitals, as
well as National Law. In the event that a medical student falls short of these expectations,
and fails to satisfactorily perform in the educational or training program, the student will be
counseled and/or disciplined for his/her actions or inactions. Outlined below is the current
course of action, that has been decided by the Leadership of the School of Medicine and
the Rectorate regarding those students who have failed, (grade: F) any course(s), or who
have a GPA less than 2.0 and according to 48th Senate decision taken on 28/2/2017 there
will be termination of studies as result of GPA lower than 1.7 by the end of year 2 (two).
Once retake exams have be graded, the Faculty of the School of Medicine will assess the
case of each individual student with a low GPA (less than 2.0) in order to determine the
appropriate course of action regarding the student’s future in the School of Medicine.
Specifically, students who received a “Letter of Probation” last year and still maintain an
unacceptably low GPA will be given only one last opportunity to correct their GPA during
the coming Semester. At the end of the Fall semester, these students (e.g. those who have
already received a letter of warning in the past), and continue to maintain a very low GPA
will receive a “Letter of Termination”, with the option to either change their program of study
(e.g. biology) or to withdraw from the school.
For those students who, on the other hand, have not yet received a “Letter of Probation” in
the past, but perform unsatisfactorily, will receive a “Letter of Probation” at the end of the
semester, with subsequent consequences should their performance not improve.
CRITERIA FOR GRADUATION OF UNDERGRADUATE STUDENTS
In order to qualify for graduation an undergraduate student must fulfill the following:
a. Complete the degree requirements in the major program as specified in the
Bulletin.
b. Complete at least the last two years or 60 credits or 120 ECTS in residence at
EUC, unless the Law provides otherwise.
c. Maintain a cumulative G.P.A. of at least 2.00 for all credits taken at EUC.
d. Settle all financial obligations to the University before certification for graduation is
granted.

September 2018 School of Medicine, EUC/Student Handbook
… 16
GRADUATION HONOURS
Bachelor degree students are identified for high academic achievement as follows:
SUMMA CUM LAUDE: Final G.P.A. of 3.85-4.00
MAGNA CUM LAUDE: Final G.P.A. of 3.65-3.84
CUM LAUDE: Final G.P.A. of 3.50-3.64
To be eligible for honours, students must complete at least 60 credits/120 ECTS at EUC.
Only EUC credits are considered in determining eligibility for such honours.
STUDENT RIGHTS, DUTIES AND RESPONSIBILITIES
This Annex describes the status of the University's students as members of the academic
community. Each enrolled student has the right to expect the University to fulfill its
educational responsibilities as effectively as its capacity and resources will permit.
Correspondingly, the University must exercise the right to establish and maintain
standards of conduct, which will promote an atmosphere conducive to learning and
meaningful individual development. Since rights carry with them certain responsibilities,
the following rights and responsibilities, institutional as well as for students, are set forth
with accompanying procedures for implementation.
BASIC RIGHTS
The following listing of basic rights is not intended to deny or limit the rights of students in
any way. Rather, it is intended to focus special attention on the rights listed because of their
importance in the educational process.
1. Free inquiry, expression, and assembly are guaranteed to all students subject to the
limitations of this document and other University regulations and policies which are
consistent with the provisions of this document and the Constitution and laws of the
Republic of Cyprus.
2. Students are free to pursue their educational goals; appropriate opportunities for
learning shall be provided by the University.
3. The right of students to be secure in their persons, papers, and effects against
unreasonable searches and seizures is guaranteed.
4. In cases involving possible sanctions of suspension, or expulsion or actions which may
place limitations on the student's right to pursue the student's educational objective,
the student shall receive prior notice of the nature and cause of the charges against
the student, shall be informed of the nature and source of the evidence presented
against the student and shall be entitled to a fair hearing before a regularly constituted
board.
Basic Duties and Responsibilities
Students, as members of the University community, shall have the following duties and
responsibilities, which are inherent in the basic rights described above:
1. The student shall have the responsibility for maintaining standards of academic
performance as established by the student's instructors.

September 2018 School of Medicine, EUC/Student Handbook
… 17
2. The student shall be responsible for acting in such a manner as to ensure other
students their basic rights as declared herein.
3. The student shall be responsible for any and all personal actions with respect to
provisions of the Cyprus law.
4. The student shall be responsible for conduct, which helps to create and maintain an
academic atmosphere, in which the rights, dignity, and worth of every individual in the
University community are respected.
5. The student shall be responsible for paying all bills owed to the University in a timely
fashion as prescribed by the University. Since Registration is not complete until all
tuition and other fees are paid, students who fail to meet their financial obligations
may have their registration cancelled; may be denied future registrations; and may
have their grades and/or transcripts withheld.
Learning Disabilities
Included are “Specific Learning Difficulties”, “Reading Disability”, by some called “Dyslexia”
and “Attention Deficit Disorder”. Central to the concept of Learning Disability (L.D.) is an
obvious difficulty in reading/reading comprehension and/or Writing/written
expression/spelling, and/or mathematical thinking. Also central is the discrepancy between
expected achievement on the basis of intelligence (especially non-verbal) and observed
achievements in these scholastic subjects.
In higher schooling and university education the disability is mostly evidenced by obvious
discrepancy between oral work and other activities of the school and written achievement,
the latter usually being lower. It is often the case that vocabulary and grammar may still be
low, compared to other students with similar capabilities.
Reading and/or writing problems may co-exist with attention deficit disorder (A.D.D.), or the
latter may be present alone. A.D.D. involves a marked difficulty in concentration, which
prevents optimum learning, and, where hyperactivity is present, the movement and
reactions of this student may disrupt the class.
CLASS ATTENDANCE
1. Students are expected to attend all classes within the formal academic schedule for
their respective semester. This requirement does not discriminate between lectures,
workshops, laboratories or clinical placements.
2. In case of an elective absence from a scheduled learning activity, students are expected
to inform the relevant instructor in written format, at least 24 hours ahead of time,
explaining the cause of absence and providing relevant documentation. Alternatively, if
not available at that time, documentation could be provided later on upon the students
return to class. In case of an emergency/unexpected absence, the relevant documents
may be submitted not later than a week afterwards. Any unjustified absence(s) may have
negative impact on the student’s participation score, the extend of which will be decided
by the respective course instructor.
3. In case of accumulated unjustifiable absences totaling to more than 3 teaching periods
for lectures and 2 teaching periods for laboratories in the same course per semester, 1
day per summer clinical orientation courses running in years 1 through 3 (the School of
Medicine has established respectively 4,5 and 6 weeks of clinical orientations/training
rotations, at the end of the academic year for the student classes of years 1,2,3 in the
General Larnaca, Nicosia and Makarios III Hospitals) and 3 days of clinical training per
course per semester in years 4 5 and 6, the student will have to justify his/her absences.

September 2018 School of Medicine, EUC/Student Handbook
… 18
It is noted that sick leaves should be justified and documented by a certified medical
doctor, otherwise, such absences will be counted as “absence periods”. Any unjustified
absences over the above range may draw remedial actions including repeat of lost
absence periods and sometimes of the entire course. This issue will be formally
discussed in a formal meeting with the instructor, the Dean and/or the Chairperson , who
will subsequently decide jointly as to whether the student may continue the course or be
given a “Fail” status which may require repetition (and potentially, a fee) of the course.
4. In any case, students are responsible for making up missed course work. Wherever
appropriate, the instructor may choose to offer supplementary classes for students with
absences. These will have to be organized so as not to disturb other learning activities
of the student or the instructor involved and the “School Council” be notified accordingly.
The attendance in such classes is also compulsory and subject to the same rules and
regulations as prior to committing the first absence incident.
5. Students will have to request permission to enter the classroom after the initiation of a
class or leave a classroom earlier but permission may be granted depending on the
instructor’s discretion. In the above cases, a student may receive an absence remark
for the particular teaching hour, based on the discretion of the respective instructor.
6. Students are expected to actively participate in all teaching activities, including
interactive learning, problem solving, case discussion and hands-on practice.
Involvement in irrelevant extracurricular activities during a teaching session may be
perceived as non-participation by the instructor, which could draw a note of an absence
at the relevant teaching hour.
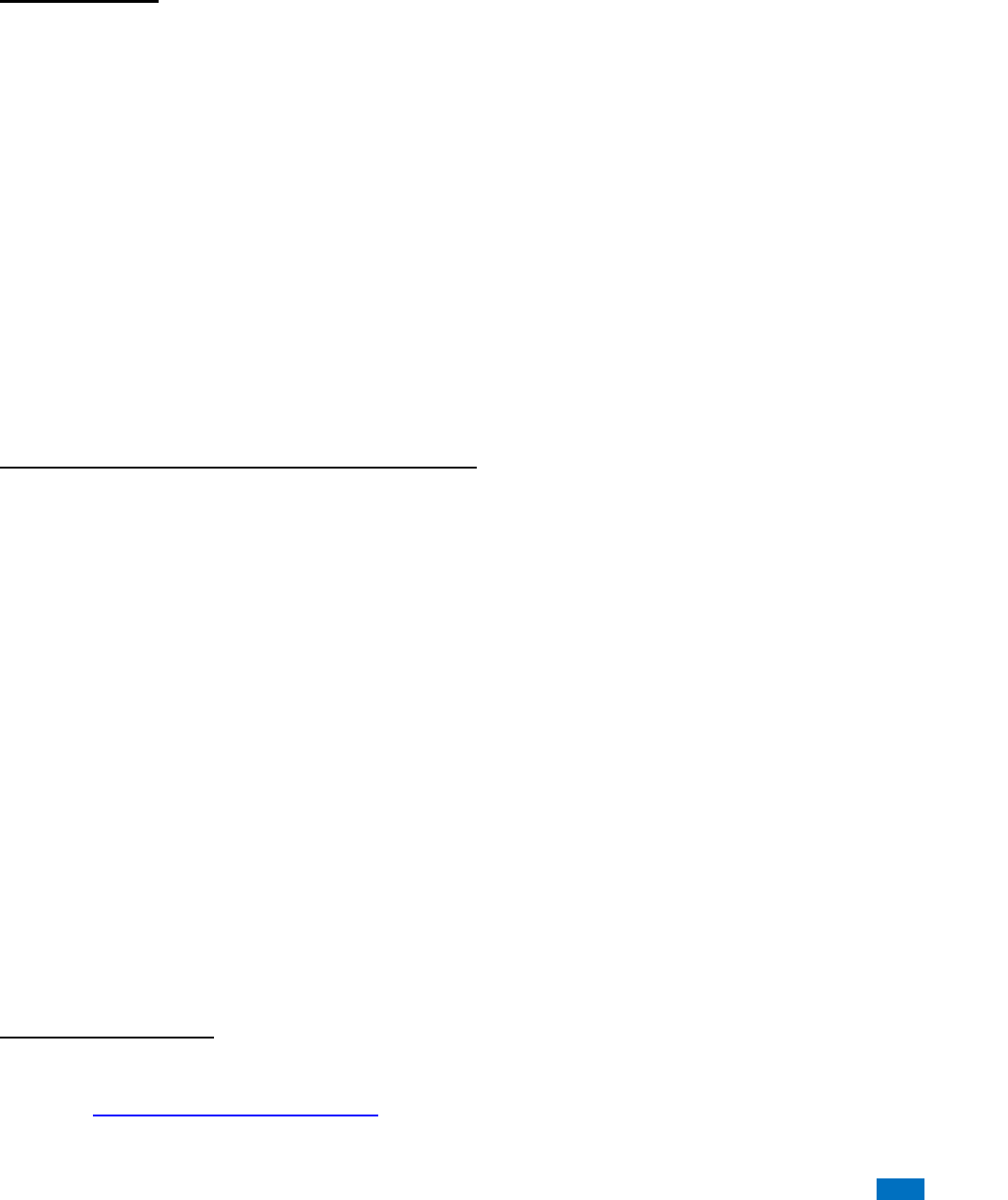
Academic Calendar
The University follows the semester/credit system of higher education and the European
Credit Transfer and Accumulation System (ECTS). The academic year consists of a Fall
and a Spring Semester, each 17 weeks long, inclusive of registration, holidays, and final
examinations. The Fall Semester begins in the last week of September, and the Spring
Semester begins a week earlier for the Medical School, due to a week break given to its
students, prior the final exams for studying.
September 2018 School of Medicine, EUC/Student Handbook
… 19

September 2018 School of Medicine, EUC/Student Handbook
… 20
SCHOOL OF MEDICINE
ACADEMIC CALENDAR
SPRING SEMESTER 2019 (28 JANUARY – 31 ΜΑΥ)
MON
TUE
WED
THU
FRI
WEEKS
JANUARY, 2019
28
29
30
31
1
1
FEBRUARY, 2019
4
5
6
7
8
2
11
12
13
14
15
3
18
19
20
21
22
4
25
26
27
28
5
MARCH, 2019
1
5
4
5
6
7
8
6
11
12
13
14
15
7
18
19
20
21
22
8
25
26
27
28
29
9
APRIL, 2019
1
2
3
4
5
10
8
9
10
11
12
11
15
16
17
18
19
12
22
23
24
25
26
13
EASTER HOLIDAYS
29
30
14
EASTER HOLIDAYS
MAY, 2019
1
2
3
14
EASTER HOLIDAYS
6
7
8
9
10
15
13
14
15
16
17
16
BREAK
20
21
22
23
24
17
FINAL EXAMS
27
28
29
30
31
18
FINAL EXAMS
SPRING SEMESTER 2019 (28/01/2019-31/05/2019)
7 January- 1 February 2019
Registration Period for the Spring Semester 2019
28 January, 2019
Opening day of instruction
15 February, 2019
Last day to make any changes in course(s) registered (ADD/DROP)
11 March, 2019
Green Monday (Public Holiday)
25 March, 2019
National Holiday
01 April, 2019
National Holiday
12 April, 2019
Last day of Withdraw & file for PASS/FAIL option from Course(s)
19 April, 2019
Last day of instruction before Easter Holidays
01 May, 2019
Labour Day (Public Holiday)
06 May, 2019
Opening Day of instruction after Easter Holidays
10 May, 2019
Last day of instruction
13 May-17 May 2019
BREAK
20 May – 31 May 2019
Final Examination period and end of Spring Semester 2019

September 2018 School of Medicine, EUC/Student Handbook
… 21
Observed Holidays
Fall Semester 2018
1. October 1
st
2018 National Holiday
2. December 24
th
2018 – January 4
th
2019 Christmas Holiday
Spring Semester 2019
1. March 11
th
2019 Green Monday (public holiday)
2. March 25
th
2019 National Holiday
3. April 1
st
2019 National Holiday
4. April 22
nd
2019 – May 3
rd
2019 Easter Holiday
5. May 1
st
2019 Labour Day (public holiday)
6. May 13
th
2019 – May 17
th
2019 Final Exams break
Student Assessment Methods
The EUC School of Medicine uses an array of various assessment methods. These
methods are different from course to course, and are clearly defined in each course outline.
The curriculum committee has approved course assessment methodologies, based on
whether they appropriately evaluate the acquisition of defined learning outcomes for the
course. Specifically, the committee ensures that the learning outcomes defined for each
course are measurable and that the assessment methods selected accomplish this
effectively. To ensure transparency, all course outlines are published on the School Website
and they are visible to everybody.
Formative Assessments
Formative Assessments e-learning are provided online (via Moodle, Blackboard) in the form
of quizzes, images, diagrams, clinical scenarios, etc. Students attempt these formative
assessment during laboratory hours.
Computer-based Interactive Quizzes During Laboratory Sessions:
Web-based quizzes are provided for the students during and at the end of the laboratory
sessions. Students are able to repeat each quiz several times and see which answers were
incorrect. The aim is for students to evaluate their knowledge and strengthen the learning
process. Instructors have computer access to the results, both during the quiz time and
afterwards. By reviewing the ongoing process, instructors are able to immediately define
any weak areas that may need reinforcement in lecture or laboratory exercises.
Summative Assessments
1- Clinical Problems (Case-based, Problem-based learning)
The clinical problem serves to integrate basic sciences with clinical thinking. Student
teams are given a clinical problem with several questions to be answered. The teams
are given one week to use their knowledge of anatomy to address the problem and
answer the questions. Students are encouraged to approach faculty from other
departments or outside physicians to discuss their clinical problem, and to search the

September 2018 School of Medicine, EUC/Student Handbook
… 22
literature. After a week, each team formally presents their findings to the entire class.
(Team grade)
2- Written Examinations:
Written examinations will consist primarily of board-level multiple choice questions
many, which entail critical thinking clinical scenarios. Short answer questions are
open ended, semi-structured questions that also incorporate foundation knowledge in
a clinical scenario.
Midterm written exam (includes material up to midterm)
Final written exam (includes material from entire semester)
3- Practical Examinations:
Practical examinations include:
1- Spot Examinations:
Interpretation of normal plain & special x-rays, Computerized Tomography
(CT) Scan, Sonogram, MRI etc. and correlate with cross-sectional anatomy of
the body
Surface marking & living anatomy
Histology slides
Developmental stages
2- Objective structured practical examination (OSPE) is also used. OSPEs are used
at assess laboratory skills with 2 station types: a procedure station, where
students are asked to perform simple structured tasks and 2) a question-based
station, where students need to analyze data and answer specific questions
related to structure & function
Components of Clinical Training Assessment
Clinical Performance
The teaching physicians who work with the student during the rotation assess the student’s
clinical performance in three areas, each of which is 20% of the grade: medical knowledge,
clinical skills and professional behavior. The more feedback the CC gets from different
members of the medical staff that instructed the student, the more objective grades can
be. The faculty assesses the extent to which the student has developed the
competencies required for that rotation. These specific competencies appear in
Section II of this manual in the curriculum for each of the core clerkships. The following
general goals form the basis of all assessments.
Medical Knowledge includes the knowledge of basic, clinical and social sciences;
the pathophysiology of disease; the clinical signs, symptoms and abnormal
laboratory findings associated with diseases and the mechanism of action of
pharmaceuticals.
Clinical Skills includes diagnostic decision making, oral and written case
presentations, history and physical examination, test interpretation and therapeutic
decision making. Students must be observed and evaluated at the bedside.

September 2018 School of Medicine, EUC/Student Handbook
… 23
Professional Behavior include the interaction with staff and patients, integrity,
sensitivity to diversity, attendance and a commitment to lifelong learning and
independent study.
Communication Skills “as they relate to physician responsibilities, including
communication with patients, families, colleagues, other health professionals and
resolution of conflicts.”
OSCEs
An objective structured clinical examination (OSCE) is designed to test clinical skill
performance and competence in skills such as communication, clinical examination,
medical procedures / prescription, exercise prescription, joint mobilisation / manipulation
techniques, radiographic positioning, radiographic image evaluation and interpretation of
results. It is a hands-on, real-world approach to learning that keeps examinees engaged,
allows them to understand the key factors that drive the medical decision-making process,
and challenges the professional to be innovative and reveals their errors in case-handling
and provides an open space for improved decision-making, based on evidence-based
practice for real-world responsibilities.
An OSCE usually comprises a circuit of short (the usual is 5–10 minutes although some use
up to 15 minute) stations, in which each candidate is examined on a one-to-one basis with
one or two impartial examiner(s) and either real or simulated (actors or electronic patient
simulators) patients. Each station has a different examiner, as opposed to the traditional
method of clinical examinations where a candidate would be assigned to an examiner for
the entire examination. Candidates rotate through the stations, completing all the stations
on their circuit. In this way, all candidates take the same stations. It is considered to be an
improvement over traditional examination methods because the stations can be
standardized enabling fairer peer comparison and complex procedures can be assessed
without endangering patients health.
As the name suggests, an OSCE is designed to be objective – all candidates are assessed
using exactly the same stations (although if real patients are used, their signs may vary
slightly) with the same marking scheme. In an OSCE, candidates get marks for each step
on the mark scheme that they perform correctly, which therefore makes the assessment of
clinical skills more objective, rather than subjective, structured – stations in OSCEs have a
very specific task. Where simulated patients are used, detailed scripts are provided to
ensure that the information that they give is the same to all candidates, including the
emotions that the patient should use during the consultation. Instructions are carefully
written to ensure that the candidate is given a very specific task to complete. The OSCE is
carefully structured to include parts from all elements of the curriculum as well as a wide
range of skills. A clinical examination - the OSCE is designed to apply clinical and theoretical
knowledge. Where theoretical knowledge is required, for example, answering questions
from the examiner at the end of the station, then the questions are standardized and the
candidate is only asked questions that are on the mark sheet and if the candidate is asked
any others then there will be no marks for them. Marking in OSCEs is done by the examiner.
Occasionally written stations, for example, writing a prescription chart, are used and these
are marked like written examinations, again usually using a standardized mark sheet. One
of the ways an OSCE is made objective is by having a detailed mark scheme and standard
set of questions. For example, a station concerning the demonstration to a simulated patient
on how to use a metered dose inhaler [MDI] would award points for specific action, which

September 2018 School of Medicine, EUC/Student Handbook
… 24
are performed safely and accurately. The examiner can often vary the marks depending on
how well the candidate performed the step. At the end of the mark sheet, the examiner often
has a small number of marks that they can use to weight the station depending on
performance and if a simulated patient is used, then they are often asked to add marks
depending on the candidates approach. At the end, the examiner is often asked to give a
"global score". This is usually used as a subjective score based on the candidates overall
performance, not taking into account how many marks the candidate scored. The examiner
is usually asked to rate the candidate as pass/borderline/fail or sometimes as excellent/
good/ pass/ borderline/ fail. This is then used to determine the individual pass mark for the
station.
Clinical Evaluation Exercise (MiniCEX)
EUC incorporates the Clinical Evaluation Exercise (miniCEX) with the Logbook framework
in order to assess clinical skills, attitudes and behaviors in the secondary care setting. By
providing a short snapshot of how students interact with patients in a secondary care setting,
it is used as an effect tool to collect evidence on competency attainment. The miniCEX is
overseen by the clinical supervisor at each hospital and may be observed by a staff doctor,
nurse practitioner, consultant or other. Observers should not be a peer or fellow clerkship
trainee.
The MiniCEX is intended to facilitate formative assessment of core clinical skills in 10- to
20- minute direct observation assessment of clerk-patient interactions. The observations
are documented in the Logbook. The aim, ultimately, is to guide clerkship learning and
improve performance through structure feedback from the clinical instructors. Particular
emphasis is place in areas such as communication, history taking, physical examination
and professional practice.
Each mini-CEX focuses on specific aspects of the clinical encounter, including:
History taking
Medical interviewing skills
Physical examination skills
Professional qualities
Counseling skills
Clinical judgment
Organization and efficiency
Direct Observation of Procedural Skills (DOPS)
Structured rating scale for assessing and providing feedback on practical procedures] will
be modified and used for complex scenarios.
Grading
EUC Medical School uses the University pass and fail marking scheme.
At the end of each semester and Summer Session, the final grades are posted in the
Students Portal, and are recorded on their permanent academic record in the Office of
the Registrar.
September 2018 School of Medicine, EUC/Student Handbook
… 25
Letter Grade
Grade Meaning
Grade Points
Percentage Grade
A
Excellent
4.0
90 and above
B+
Very Good
3.5
85-89
B
Good
3.0
80-84
C+
Above Average
2.5
75-79
C
Average
2.0
70-74
D+
Below Average
1.5
65-69
D
Poor
1.0
60-64
F
Failure
0
-
I
Incomplete
0
-
W
Withdrawal
0
-
P
Pass
0
-
AU
Audit
0
-
TR
Transferred
0
-
The grade “I” is awarded where a student has maintained a satisfactory level of performance
but was unable to complete a major portion of course work (e.g. term paper or final exam),
for reasons deemed acceptable by the instructor. It is the responsibility of the student to
justify any failure to complete work required, and to reach an agreement as to how
remaining course requirements will be satisfied. Following the award of an “I” mark and in
consultation with the course instructor, the student is responsible for fulfilling any
outstanding course requirements within the first weeks of the following semester. In
exceptional cases, the instructor may extend the existing incomplete grade to the next
semester. Failure to complete work within a specified period will result in an “F”, which will
be recorded as the final grade.
In the case where a student believes that the grade received is different from what was
expected, the EUC Charter defines the procedure for appeals. Specifically, the student
must exhaust all possibilities of resolving the problem with the pertinent instructor first. If
this does not lead to a resolution, the student may appeal against the grade by filing a
petition with the Office of the Registrar. The Registrar will forward a copy of the petition to
the pertinent Chairperson of Department, who will first ascertain that no error was made by
the instructor, and if so will assign an anonymous re-evaluation of the final
examination/project to another instructor. In the case of major discrepancy between the
instructor’s evaluation and the re-evaluation that will require change of grade, the average
of the two evaluations will be assigned as the final grade to the final examination/project.
Changes of grades resulting from an appeal require the endorsement of the Dean of School.
For a petition to be reviewed, a student must appeal within four (4) weeks from the date the
results are announced.
Appeal / Grievance.
A committee consisting of a high-rank academic administrator, a high-rank faculty member
and a high-rank external member will investigate all appeals / grievances.

September 2018 School of Medicine, EUC/Student Handbook
… 26
Remediation Policy for Absentees or Low GPA
The School of Medicine expects all medical students to fulfill their responsibilities and
conduct themselves in a competent, professional manner, and to follow the rules,
regulations and policies of the European University of Cyprus and affiliated hospitals, as
well as National Law. In the event that a medical student falls short of these expectations,
and fails to satisfactorily perform in the educational or training program, the student will be
counseled and/or disciplined for his/her actions or inactions. Outlined below is the current
course of action that has been decided by the Leadership of the School of Medicine and the
Rectorate regarding those students who have failed (grade: F) any course(s), or who have
a GPA less than 2.0 and according to 48th Senate decision taken on 28/2/2017 there will
be termination of studies as result of GPA lower than 1.7 by the end of year 2 (two).
Once retake exams have be graded, the Faculty of the School of Medicine will assess the
case of each individual student with a low GPA (less than 2.0) in order to determine the
appropriate course of action regarding the student’s future in the School of Medicine.
Specifically, students who received a “Letter of Probation” last year and still maintain an
unacceptably low GPA will be given only one last opportunity to correct their GPA during
the coming Semester. At the end of the Fall semester, these students (e.g. those who have
already received a letter of warning in the past), and continue to maintain a very low GPA
will receive a “Letter of Termination”, with the option to either change their program of study
(e.g. biology) or to withdraw from the school.
For those students who, on the other hand, have not yet received a “Letter of Probation” in
the past, but perform unsatisfactorily, will receive a “Letter of Probation” at the end of the
semester, with subsequent consequences should their performance not improve.
Section II: Academic & Clinical Requirements for MD Program
Curriculum
Overview of the Three-Phased Integrated-Spiral Program
The modules for each Structure & Function Unit are briefly described below, to underscore
the integration ladder throughout the basic science years of study to the clinical trainings.
Horizontal integration brings together the various disciplines (e.g. Anatomy, Histology,
Embryology, Physiology, Biochemistry) for each module, whereas vertical integration is
aimed at bringing together basic and clinical sciences, in order to break the traditional divide
between preclinical and clinical studies. As such, the knowledge presented in the basic
sciences is placed in clinical context and in context of professional practice. The overall
aim is to enhance the acquisition of knowledge, skills, attitude, values and professionalism
in our students.
Each Unit incorporates multiple teaching modalities, including lectures, case-based
learning, team-based learning, problem oriented patient sessions (POPS), laboratories,
patient skill laboratories, simulation, computer-assisted learning (CAL), among others.
Regular formative assessments, similar to those used at the end of the unit summative
assessments, will help students track their progress.

September 2018 School of Medicine, EUC/Student Handbook
… 27
Phase I: Foundations of Medicine (Years 1 -2)
Foundations of Medicine (Phase I) are provided across the first two years of medical
education. During this time, students develop the foundational understanding and skills
necessary to understand disease processes that will be taught in Phase II (Foundations
of Clinical Practice) and begin to care for patients during their medical clerkships (Phase
III: Clinical Medicine Core). Students begin to form their professional identity from day
one, as they learn clinical skills, foundational medical knowledge, and the skills needed to
develop into life long learners.
The interdisciplinary units in the Foundations of Medicine phase of the curriculum use a
multidisciplinary, systems-based, horizontally integrated approach to teach the
normal structure and function of the body, along the continuum from molecules-to-cell to
entire functional systems. During this process, students are also introduced students to
basic clinical skills, and abnormalities in structure and function, when appropriate. The
disciplines (Cell & Molecular Biology, Biochemistry) and (Anatomy, Histology-Embryology,
Physiology, Biochemistry) are integrated and organized into modules based on foundational
concepts or on organ systems. The teaching of communication skills is also fully integrated
alongside and introduction to the demands of professional practice and care.
Structure & Function: From Molecules to Cells
Year 1, Semester 1
Courses:
1. Cellular & Molecular Biology
2. Medical Biochemistry I
3. Physics for Biomedical Sciences
4. Introduction to Epidemiology
5. Biostatistics
The first semester presents the basic principles of human biochemistry, cellular & molecular
biology and will provide the foundation knowledge to understand the biochemical,
molecular, cellular and genetic basis for disease. The courses of this unit proved a wide-
range of scientific knowledge that underlies medical practice drawn from biochemistry,
genetics, cell biology, molecular biology, etc. This semester includes active-learning
components such as simulation lab exercises, small-group instruction and TBL. Also
included in this unit is physics for biomedical science, biostatics and an introduction to
epidemiology. The later help students’ master medical information.
Structure & Function: Body System in Health I
Year 1, Semester 2
(Musculoskeletal, Integumentary, Hemopoietic, Lymphatic, Endocrine, Exocrine
Systems)
Courses:
1. Anatomy I
2. Histology-Embryology I
3. Physiology I
4. Medical Biochemistry II
5. Introduction to Genetics

September 2018 School of Medicine, EUC/Student Handbook
… 28
6. Clinical Practicum I
The second semester will begin with an overview of major body systems, and early
development. Integration of disciplines (anatomy, histology, embryology, physiology and
biochemistry) will address the introductory principles, the musculoskeletal system,
integumentary system, hemopoietic-lymphatic systems, and endocrine/exocrine systems.
Throughout the term, students will apply practical (clinical) skills and incorporate new
information related to examination of the patient including Adams bending test for spinal
deformities, palpation of bony landmarks, muscle function examination, among others.
Structure & Function: Body System in Health II
Year 2, Semester 1
(Organ Systems)
Courses:
1. Anatomy II
2. Histology-Embryology II
3. Physiology II
4. Human Nutrition & Metabolism
5. Family Medicine – Public Health
The second part of the Structure & Function Body Systems in Health integrates disciplines
(anatomy, histology, embryology, physiology and biochemistry) to address primary organ
system structure and function (e.g. cardiovascular, respiratory, digestive, urinary and
reproductive systems). Among the topics covered are energy generation by metabolism of
basic foodstuffs, and the role of nutrition in health and disease, as well as homeostasis. The
overview of major organ systems will allow students to begin learning and practicing basic
clinical skills, such as listening to heart and lung sounds, palpation of major organs and
measuring pulse and respiration rates. Learning will be supplemented by the use of medical
imaging, such as radiographs, CTs, MRIs and ultrasound. Students will explore the structure
of the organ systems and the physiology underlying their normal function, and relate the
development and anatomy of the organs to their microscopic structure and the mechanisms
underlying functionality. Students will learn how their functions are integrated and what
happens when this normal state is disrupted. Throughout the Unit students will apply
practical (clinical) skills and incorporate new information related to examination of the
patient including ECG data interpretation, listening to heart sounds and imaging techniques.
Structure & Function: Body System in Health III
Year 2, Semester 2
(Mind, Brain & Behavior)
Courses:
1. Neuroscience
2. Medical Psychology
3. Basic Immunology-Microbiology
4. Introduction to Clinical Skills
5. Major Elective

September 2018 School of Medicine, EUC/Student Handbook
… 29
This is the third unit of the structure & Function of Body Systems in Health, which is devoted
to understanding the central nervous system. Medical Neuroscience is an integrated
course, which integrates neuroanatomy, histology, embryology, physiology and
biochemistry to understand the structure and function of the central nervous system.
Students will examine the gross and microscopic structures of the various regions of the
human brain, using models, imaging and virtual microscopy. Students will learn to apply
concepts of central neural pathways to the neurological aspect of the physical examination,
and will explore how the brain determines aspects of human behavior and consciousness
and the consequences of defects that lead to abnormal function.
This unit also introduces students to the basic defense systems of the human body.
Appropriate, since the immune system has been considered the “floating brain”. Students
will learn basic immunological principles and their clinical relevance. They will be introduced
students to infectious diseases, the biology of the causative agents and the defense
systems that protect against them.
This term students will be introduced to clinical skills related to taking a medical history
and performing a physical exam.
Clinical Training Spiral
1st year – Foundations of Medicine I are taught in modules that cover traditional synergies
related to understanding the Structure and Function of the human body from molecules to
cells (e.g. cell biology, biochemistry, genetics), as well as medical information
(epidemiology, biostatistics) in the first term and the basic structural components of the
human body (anatomy, physiology, histology, embryology, biochemistry) in the second
term. Students are given their first introduction to clinical practice in «Clinical Practicum».
2nd year – Foundations of Medicine II are taught in modules that cover traditional
synergies related to understanding the structure and function of the human body (anatomy,
physiology, histology, embryology, biochemistry) that is organized in primary body systems
(cardiovascular, pulmonary, renal reproductive and nervous). Instruction of basic clinical
skills are promoted via the course and practicum in «Introduction to Clinical Skills», as well
as by the use of simulated scenarios.
3rd year – Foundations of Clinical Practice focus is on pathophysiology, formation of
differential diagnoses, semiology, pathology and pharmacotherapy that is also organized in
body systems over the course of the year. Basic clinical skills are further promoted via
simulation. Students are also introduced to general surgery, immunology and microbiology.
4th-6th years – Clinical Medicine Core forms the final turn of curriculum spiral, with the
translation of knowledge and skills into practice, during clinical clerkships.
Themes such as medical ethics, family medicine, public health, etc. span all years and are
threaded throughout the basic modules and clinical clerkships.
The curriculum of the School of Medicine, European University Cyprus (EUC) is of total
duration of 5685 hours and includes theoretical and clinical training, according to the
European Directive 2013/55/EU of the European Council. Students’ clinical training is an
integral part of their education, of total duration of more than 2200 hours. Clinical training

September 2018 School of Medicine, EUC/Student Handbook
… 30
takes place in pre-determined sites of the public and private sector, following appropriate
planning.
The overall objectives of the clinical training of medical students are:
To familiarize students with the structure, function and capacities of the healthcare
system
To develop clinical skills and successfully combine them with their theoretical
knowledge
To demonstrate and develop communication skills and teamwork
To apply practical skills in real-life healthcare environments
To develop professionalism in their daily clinical practice
To establish the concept of clinical training during medical undergraduate studies
To create an environment of mutual collaboration and develop ongoing relations
between the School of Medicine and the collaborating healthcare sites
Finally, to equip medical graduates with all necessary practical skills to pursue their
postgraduate endeavors
The Clinical Curriculum (Years 4-6, Semesters 7-12)
Core Rotations
ECTS
Weeks
Clinical Training I
(Respiratory & Cardiovascular)
15
6
Clinical Training II
(Digestive System & Hematology)
15
6
Clinical Training III
(Infectious Diseases and Clinical Microbiology)
9
3
Clinical Training IV
(Endocrine system, Uro-Nephrological System &
Male Genital Tract)
14
6
Clinical Training V
(Musculoskeletal System)
7
6
Clinical Training VI
(Nervous System & Psychiatry)
15
6
Clinical Training VII
(Pediatrics)
12
5
Clinical Training VIII
(Dermatology)
6
2.5
Clinical Training IX
(Obstetrics & Gynecology)
8
3

September 2018 School of Medicine, EUC/Student Handbook
… 31
Clinical Training X
(Ophthalmology)
6
2.5
Clinical Training XI
(Otorhinolaryngology)
5
2.5
Clinical Training XII
(ER, Toxicology, Oncology & Palliative Care)
14
5
Additional Requirements
Diagnosis by Imaging
7
2
Clinical Bioethics & Legal Medicine
6
2
Medical Therapeutics
6
1.5
Symptoms & Interpretation Of Complementary
Examination Procedures
5
1.5
Primary Care
6
3
Electives
Healthcare Management
Clinical Embryology
Rehabilitation Medicine
Research Methods & Scientific Writing
Interventional Radiology
Medical Student Competencies
The US Accreditation Council on Graduate Medical Education (ACGME) defines six
domains thought to be useful in defining “competency”; these are called the core
competencies - patient care, medical knowledge, practice-based learning and
improvement, professionalism, systems-based practice, and interpersonal skills and
communication. While these were initially developed for residency programs, today
competencies are used at many levels of professional practice to define and measure
an individual’s ability and capability. EUC has devised a Clinical Competence Building
Roadmap to guide both instructors and students during their clerkships. (Appendix VI)
September 2018 School of Medicine, EUC/Student Handbook
… 32
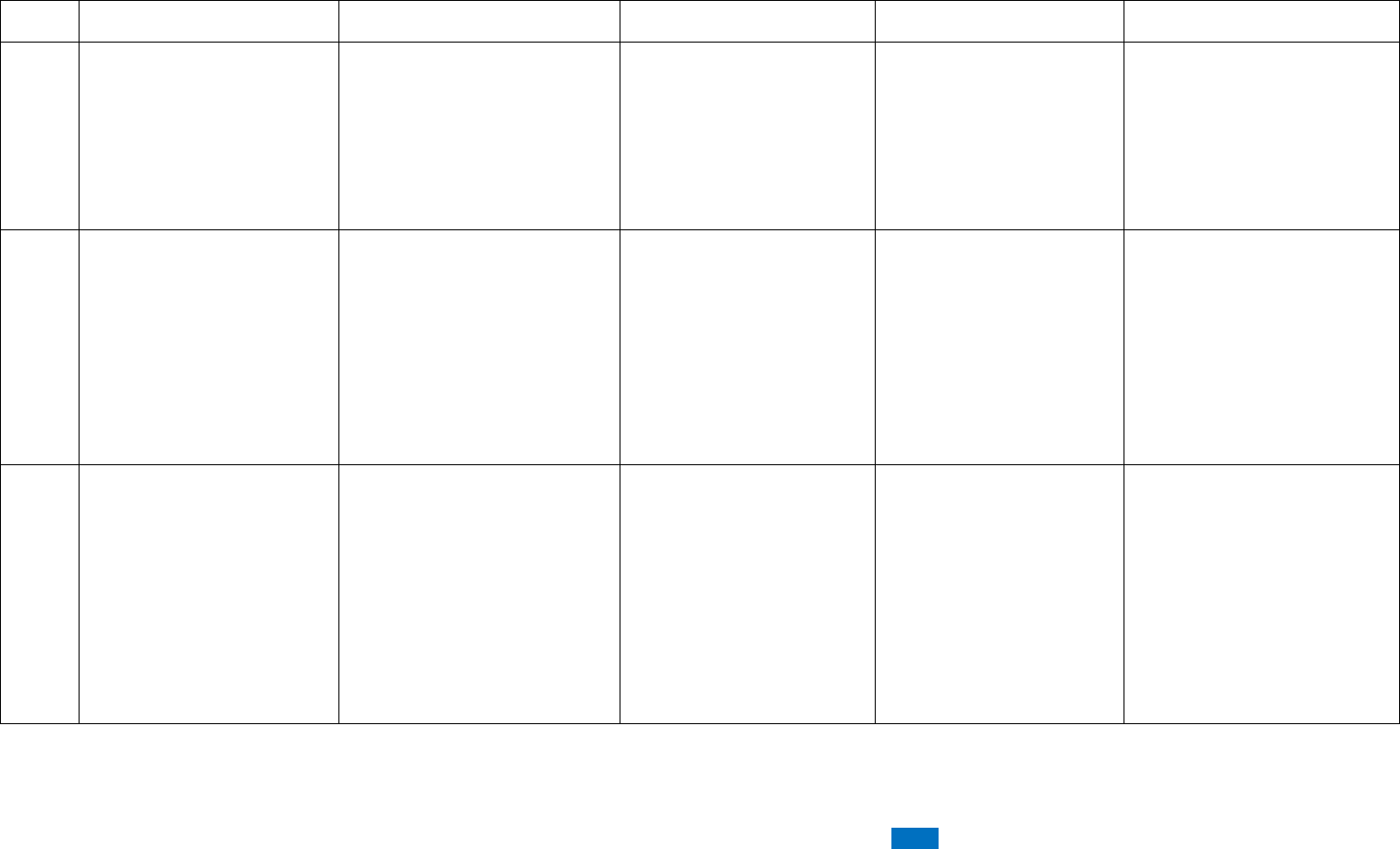
Clinical Competence Building Roadmap
Year
Knowledge
Attitude
Skills
Milestone
Deliverables
1
Structure And Function –
Human Body In Health
Introduction To Patient-
Doctor Relationship
Health And Safety
Hand Hygiene
Glove Use/Disposal
Initiating Medical
Interview
Vital Signs
Multicultural And
Interdiscplinary
Communication
Graded Mpr101 Course
– First Clinical
Orientation Visit Plus
Ward Simulation
Workshops
-Year 1 Logbook
-Recorded Video Sessions
On Interdisciplinary
Communication
-Written Assessment On
Clinical Communication
Problems
2
Structure And Function –
Human Body In Health
And Structured Approach
To The Patient (Transition
Year)
Dealing With Conflict/Anger
Working With Teams
Recognizing Opportunities
For Prevention And Health
Promotion
Nutritional Screening
History Taking
Ecg Recording
Physical Examination Of
A Healthy Patient
Venous Blood Sampling
Iv Catheterization
Abgs
Sc/Im Injections
Mantoux Test
First Clinical Placement
In Primary Care In
Semester 3 /
First Formative Osce In
Semester 4
-Year 2 Logbook
-Recorded Video Sessions
On Team Work And History
Taking
-10 Completed History And
Examination Sets
3
Structure And Function –
Human Body In Disease
Breaking The News
Passing Information
Suturing
Wound Care
Iv/Io Placement
Ngt/Peg Insertion
U/C Placement
Intubation/Airway
Management
Recognizing Abnormal
Signs/Symptoms
Performing Basic
Differential Diagnosis
Formative And
Summative Osce In
Each Semester
Optional Certification In
Bls
-Year 3 Logbook
-Recorded Video Sessions
On Complete
Primary/Secondary
Assessment Stations

September 2018 School of Medicine, EUC/Student Handbook
… 33
4
Core Clinical
Competences – Adults
Triage / Assessing Patient
Severity
Conducting A Structured
Clinical Approach (From
History To Treatment)
Managing Intimate
Examinations
Using Decision Support
Algorithms And Scores
Diagnosis And
Treatment:
Cardiovascular /
Respiratory / Gi / Blood
And Lymphatics / Urinary
And Endocrine System
Obtaining Cultures
Appropriate Choice And
Interpretation Of
Common Imaging
Modalities
Opportunity For Elective
Clinical Rotations In
Coooperating Hospitals
Abroad
-Year 4 Logbook
-Use Of Mini Cex And Dops
As Assessment Tools In
The Clinics (Wpba)
5
Core Clinical
Competences – Mental
And Child Services
Clinical Approach To Non
Cooperative Patients
(Minors, Mental Disability)
Bioethical Considerations
Diagnosis And
Treatment:
Musculoskeletal /
Nervous System And
Skin, Mental And
Children’s Health
-Year 5 Logbook
-Use Of Mini Cex And Dops
As Assessment Tools In
The Clinics (Wpba)
6
Core Clinical
Competences – Mother
Health And Emergencies
Multicultural Approach To
Care
Dealing With Disability
(Sensory/Motor/Cognitive)
Breaking The News (Death /
Cancer / Toxic Agent Use /
Abortion / Stillbirth)
Working In Teams In
Stressful Conditions (Crisis
Management)
Diagnosis And Treament:
Reproductive System,
Eye And Ent Conditions,
Poisonings And
Emergencies
Observation Of Advanced
Skills (Lp, Cvc, Chest
Tube, Biopsy)
Clinical Elective
Free Electives In Both
Semesters With A
Potential Research
Direction
Eligibility For Als/ Atls /
Phtls Accreditation
Usmle Exam (To
Practice In Usa)
-Year 6 Logbook
-Lpa Assessment
-Use Of Mini Cex And Dops
As Assessment Tools In
The Clinics (Wpba)
-Completion Of Individual
Portfolio For Residency
Applications
-Graduation / Issue Of
Medical License

September 2018 School of Medicine, EUC/Student Handbook
… 34
Entrustable Professional Activities (EPAs)
The American Association of Medical Colleges (AAMC) has grouped competencies into the
following 13 Entrustable Professional Activities (EPAs) as a basis for starting
postgraduate training in the US.
1. Gather a History and Perform a Physical Examination
2. Prioritize a Differential Diagnosis Following a Clinical Encounter
3. Recommend and Interpret Common Diagnostic and Screening Test
4. Enter and Discuss Orders/Prescriptions
5. Document a Clinical Encounter in the Patient Record
6. Provide an Oral Presentation of a Clinical Encounter
7. Form Clinical Questions and Retrieve Evidence to Advance Patient Care
8. Give or Receive a Patient Handover to Transition Care Responsibility
9. Collaborate as a member of an Interprofessional Team
10. Recognize a Patient Requiring Urgent or Emergent Care, & Initiate Evaluation &
management.
11. Obtain Informed Consent for Tests and/or Procedures
12. Perform General Procedures of a Physician
13. Identify System Failures and Contribute to a Culture of Safety and Improvement.
The emphasis of the EUC curriculum is on achieving and demonstrating competency.
Student confidence in performing practical and clinical skills is assessed by using a student
questionnaire (Appendix VII).
Team Based Learning (TBL)
TBL will be applied in all S&F courses. It serves to move the courses away from one-way
lecture style, to a more interactive and engaging instruction. The aim of TBL is transform
students from passive information receivers, to active collaborators working with each other
to learn how to use concepts and course material in practical situations. TBL is a “Learn
by doing”, rather than a “learn by listening approach”. This teaching tool helps students
form self-supported, collaborative & cohesive learning groups. The approach is based on
the premise that interactive group collaboration improves the quality and resonance of
students’ shared learning experiences. Students don’t just hear about core concepts, but
rather learn how to use these concepts. By collaborating in teams, students develop
analytical and empathetic behavioral skillsets, as well as understand the importance of
accountability, responsibility and professionalism. All of these skills and attitudes provide
practical and valuable advantages for the student later in their career. The effectiveness of
TBL is based on long-term learning, learner accountability, incentivized collaboration and
frequent learning application feedback.
Practicalities: TBL is used at EUC to allow us to shift towards conceptual understanding
to applied use of knowledge in:
Practical laboratory exercises
Simulation scenarios
Clinical Problem/Case Solving & Discussions

September 2018 School of Medicine, EUC/Student Handbook
… 35
Clinical Problem Presentations
From the onset of the semester, students are divided into teams of 4 to 6 students who will
work together during laboratory sessions and clinical problems. Each team selects a team-
leader. Group schedules are managed by the professors and are maintained throughout
the entire semester. Students are then accountable for coming to laboratory sessions
prepared and contributing value to their team. Professors provide immediate & frequent
feedback on how students are actually applying concepts.
Self-Directed Learning – Computer Assisted Learning
Computer-Assisted Learning (CAL): augments, enhances and improves instruction of all
structure and function modules. It promotes independent learning, problem solving, and
allows schedule flexibility. The increased collaboration between disciplines has led to
advances in anatomical informatics, three-dimensional modeling and virtual reality
methodology, which in turn, have made computer-based structural visualization a new and
practical tool for structure and function education. The value of CAL is that it allows
individual students to learn at their own personal pace. 3D engagement tools provide
interactive models of the human body for students using the web browsers provided in the
computer lab or mobile apps. To enhance our educational program at EUC, computer-
based instruction and other interactive computer-related activities have been effectively
integrated into the total instructional process.

September 2018 School of Medicine, EUC/Student Handbook
… 36
Section III: Student Resources
Library
The Library of the European University Cyprus strives to maintain not only a level of
academic excellence but also of flexibility in order to be among the first to adopt to the
changes that take place in regards to traditional teaching and teaching methodology. It is
due to this flexibility why the library of EUC (as Cyprus College) first offered online
access to a Library webpage in Cyprus and through the webpage to thousands of
other sites. Additionally the library added its first electronic journals database in 1996
(Gale’s SearchBank/Infotrac) and was one of the first to offer in Cyprus access to
Proquest’s ABI/Inform and Emerald’s Management Insight through its internet
facilities.
The Library is located on the second floor of the South Block Building. It occupies the whole
floor and has a total area of 1300 square meters. The Library has a seating capacity of
approximately 160 persons.
The university Library is centrally heated and air-conditioned in order to enhance the
learning environment of the University. The Library has a Reference Desk (used as an
office area for the five librarians), a section of current periodicals, a book collection, a display
area for new books and periodicals. The Library is fully computerized in order to assist
librarians and students in a variety of ways. Computer terminals are available for the users
providing access to the Internet. There are 17 public workstations supporting the needs of
users, 3 stations for searching the Library’s cataloguing system and 1 station used by the
librarians in assisting users and providing training courses. In addition, the library has a
computer lab with twenty stations, 2 study/presentation rooms with a sitting capacity for 10
users for each room, and a photocopy room with two machines. Finally, there is a Self
Service Station by Nedap library, which contains a barcode, Mifare or RFID reader to
identify the user, an RFID reader for the check-in/out process and a touch screen for user
interaction. Additionally, the Self Service Station contains a printer for the receipts. The Self
Service Station functions as a check-in/check-out combi station.
Located next to the library, as a separate entity, is a reading room with a capacity for 50
students. The reading room has an extended time schedule since it stays open from
8:00a.m. to midnight, seven days a week.
Moodle
Moodle is European University’s learning management system (LMS). Developed from a
learning-centric perspective rather than a technical administrative perspective, Moodle
enables faculty members to enhance their face-to-face teaching and their students’ learning
by providing an online environment to distribute materials and encourage collaboration and
interaction both within and outside the classroom.

September 2018 School of Medicine, EUC/Student Handbook
… 37
USMLE Services
Web-portal
EUC School of Medicine meets the requirements established by Educational Commission
for Foreign Medical Graduates (ECFMG), giving opportunity to EUC students and
graduates to apply to ECFMG for Certification and Examination in the USA. To facilitate
our students who are interested in applying for post-graduate and residency programs in
the USA, the Department of Medicine has also established an ECFMG Medical School
Web Portal (EMSWP), which gives us full access to the ECFMG services for international
medical students.
For EUC students who are interested in USMLEs and Residency/Post-graduate programs
in the USA, access to the following services is provided:
• Status Verification: verify the status of EUC students/graduates who apply to ECFMG
for Unites States Medical Licensing Examination (USMLE). The ECFMG
Certification – assess whether our International Medical Graduates (IMGs) are
ready to enter US graduate medical education programs that are accredited by the
Accreditation Council for Graduate Medical Education (ACGME). ACGME requires
that all international medical graduates who enter ACGME-accredited programs to
be certified by ECFMG. ECFMG Certification assures directors of accredited
residency and fellowship programs, that international medical graduates have met
the standards of eligibility.
• Credentials Verification: verify the authenticity of the medical education credentials of
EUC students & graduates. [We can verify medical credentials provided by ECFMG;
send credentials and their verifications to ECFMG; and/or provide information on
graduates’ medical education requested by ECFMG.] The Certification
Verification Service – provides the primary-source for confirmation of ECFMG
certification status to residency programs, state medical boards, and other
organizations, such as hospitals and HMOs.
• Performance Data: EUC can obtain information on the performance of our
students/graduates on Step 1, Step 2 clinical Knowledge, and Step 2 Clinical Skills
of USMLE.
• ENSWP Electronic Residency Application Service (ERAS): EUC can now submit
ECFMG supporting documents and tack receipt n behalf of our students/graduates
who are participating in the Electronic Residency Application Service (ERAS).

September 2018 School of Medicine, EUC/Student Handbook
… 38
USMLE Examination Preparation
The purpose of this program offered by the EUC is to facilitate this process by providing
resources for targeted exam preparation over a total of 3 weeks. Instructions will be
provided through 4 lecture units per day covering USMLE 1 and USMLE 2-CK topics one
week each. High-yield topics will be selected for specific review, which will be adjusted every
cycle. Furthermore, students have access to online question catalogues allowing them to
practice newly acquired knowledge. A third week will be dedicated to the specifics of the
USMLE 2-CS examination, which requires to perform physical examination and
communication with patients and colleagues. The remainder of the third week will be
dedicated to introducing the residency application process through the “Match” (National
Resident Matching Program (NRMP).

September 2018 School of Medicine, EUC/Student Handbook
… 39
Section IV: Student Health & Services
Health Requirements
Health Requirements for Clinical Rotation
Students need to have all mandatory health requirements completed, documented and
cleared, before they can start their clinical rotation. Students must send all documents to
the office of the Clinical Training Committee, Eva Charalambous, Administrator at
EUC health requirements include:
TB SCREENING AND IMMUNIZATION RECORD
A. TUBERCULOSIS SCREENING
Screening consists of a 2-step skin PPD test or an interferon gamma release assay blood
test, e.g. QuantiFERON - TB Gold within 1 year prior to the start of their rotation.
B. MANDATORY IMMUNIZATIONS
1. Measles, mumps, rubella
Students are required to submit either a history of 2 doses of MMR (measles,
mumps, rubella) vaccination or laboratory copies of sufficient serum IgG titers
for measles, mumps, and rubella. If any of the serum IgG titers indicated non-
immunity, students must submit evidence of a MMR vaccination obtained after
the non-immune titer date.
2. Hepatitis B
Completion of the hepatitis B series (3 vaccinations) is a mandatory requirement.
Students need to submit the dates of vaccination and the results of a serum
hepatitis B surface antibody test obtained after the series was completed. If the
hepatitis B titer result indicates non-immunity, students should submit proof of one
additional vaccine after the titer result date. Students should also check with their
personal physician who may advise further vaccines and titers.
1. Tdap vaccination within ten years is mandatory
C. ADDITIONAL VACCINATIONS
Depending on the clinical training site, students might also need to review the health form
recommendations for other vaccinations (eg.polio, hepatitis A, varicella zoster, influenza).
D. ANNUAL REQUIREMENTS
After starting clinical training, and to continue, students will be required to submit the
following on an annual basis:

September 2018 School of Medicine, EUC/Student Handbook
… 40
1. Tuberculosis screening (as described above)
2. Any changes in their immunization history.
Student Health and Safety
Compliance with health and safety measures is necessary for the proper function of clinical
training. These measures concern safety of students, of healthcare workers, of patients and
their chaperones.
When concerned over a safety issue or an incident, students should contact their Clinical
instructor, Department Clinical Coordinator and/or Hospital Coordinator of Clinical
Education. In case of personal safety issues, such as injury or exposure, students should
also immediately contact the CTC, either directly or through the Health and Safety Officer.
The student Logbook contains details on student safety matters. In addition, the Clinical
Practice Incidence Report Form (Appendix IV) should be completed and submitted to the
School, in case of any incidence concerning student safety.
Immunization
Before entering the clinical training and in order to approve their entry in healthcare settings,
students should conform to the immunization requirements set by the Ministry of Health
(See above)
Hand hygiene and isolation precautions
Standard precautions and Hand hygiene are performed before and after contact with
all patients. Indications and technique for hand hygiene follow the World Health
Organization guidelines.
Isolation precautions, personal protective equipment are additional measures that
depend on the risk of transmission between patients and healthcare personnel (i.e.
contact, droplet, and airborne precautions).
Gloves are worn for invasive procedures, contact with non-intact skin, mucous
membranes, or sterile sites, and at all activities that carry risk of exposure to body
fluids or contaminated instruments.
Safe use and disposal of sharps
Incidents with sharps injuries can be prevented with basic practices:
Do not pass sharps directly from hand to hand
Always discard in appropriate sharps container immediately after use
Do not break or bend needle
Container should be kept within arms’ length during use
Do not attempt to replace cap

September 2018 School of Medicine, EUC/Student Handbook
… 41
Counseling and Mental Health Support
The School of Medicine of the EUC is committed to provide to students scientific excellence
and education. Our aim has been to address the multiple needs of students to support them
throughout their academic journey. Studying abroad constitutes a major transition in student
life. This is further challenged by the high academic standards of studying Medicine. The
underpinning philosophy of our School stems from the fundamental values of the World
Health Organization about health and wellbeing, emphasizing the role of physical, mental
and social health in academic achievement and later life. Congruent with this, we have
developed a network of academic and mental health services and resources so as to
facilitate our students adapt to the new academic environment, enhance their capacity to
personal autonomy and independence and provide additional help to those facing increased
stress levels, learning difficulties and other psychosocial problems which are often
associated with poor academic performance.
Many students hesitate to disclose their difficulties to universities due to fear of
discrimination; however, mental health difficulties are extremely common. There is no
standard definition of what constitutes a mental health difficulty. It may include disorders
such as depression, anxiety (e.g. panic attacks) as well as schizophrenia, bipolar disorder,
obsessive-compulsive disorder (OCD), eating disorders, self harm or even difficulties such
as sleeping problems, high stress levels, difficulties in concentration, studying, fail to follow
the schedule etc.
Mental health difficulties are more common than we think. Conditions like depression and
anxiety count for at least half of the general practitioners visits than any other physical
condition. It is estimated that one in four individuals worldwide seek help for mental health
problems every year. Our mental health is affected by multiple factors and can be triggered
by transitions or stressful events and periods that make us more vulnerable. Mental health
problems can be successfully tackled as long as we seek for adequate, appropriate and
effective care. Thus, we would like to invite our students to share their academic and mental
health concerns with us, at any stage of their academic life: before the admission process,
after recruitment, at any level of their studies. All students are treated equally independently
of their socio-cultural background, gender, preferences, and physical and mental health
difficulties. We value the social diversity and we use mentoring and support to promote the
multicultural character of our school.
Students can ask for an appointment with academic counselors to disclose their fears,
difficulties and mental health problems. They should expect to:
a) Be treated equally
b) Have some discussion about the nature of their difficulties and how they interfere
with their academic performance
c) Develop a plan for action. The plan is mutually developed by the academic counselor
and the student and may include counseling, study-groups, referral to mental health
professional and reasonable adjustments so as to tailor the academic requirements to
the student needs so as to ensure an optimal academic life.
Special Counselor: Dr. Irini Agapidakι
We are committed to build an inclusive and supportive academic community that
supports equality of opportunity for everyone.

September 2018 School of Medicine, EUC/Student Handbook
… 42
Section V: Course Catalog & Descriptions
Foundations in Medicine Year 1
MED101 Medical Biochemistry I
Course
Coordinator
Patrikios I., Professor
Instructors
Dimas C., Scientific Collaborator
Calder P., Professor, Visiting Faculty
Credits
3
Hours
Lecture : 3
Practical : 4 (Laboratory/Clinic)
Offered
Fall Semester
Description
The objective of the course is to familiarize the students with the Molecular
bioavailability, metabolism, storage and biosynthesis of micro and macro
molecules and the regulation of their pathways. Description of the biochemical
basis of inherited disorders with their associated sequelae of various
metabolisms. Description of blood and urine metabolites and their importance
in health and disease.
MED102 Cellular & Molecular Biology
Course
Coordinator
Stephanou A., Professor
Instructors
Politis P., Scientific Collaborator
Credits
3
Hours
Lecture : 3
Practical : 4 (Laboratory/Clinic)
Offered
Fall Semester
Description
This course is intended to give the student a broad overview of cellular and
molecular biology with respect to human cells. It is designed to acquaint
students with the fundamental terms, concepts, and principles of the
functioning of human cells in normal and abnormal states. The course will
prepare the students to be more familiarized with their courses in cellular
physiology and cellular histology. A key part of the course will be the ability to
dissect problem scenarios into its key features by thinking in an integrated
manner and to looking at problems from different perspectives.

September 2018 School of Medicine, EUC/Student Handbook
… 43
MED103 Physics for Biomedical Sciences
Course
Coordinator
Polycarpou I., Lecturer
Instructors
Kaplanis P., Scientific Collaborator
Credits
3
Hours
Lecture : 4
Practical : 0 (Laboratory/Clinic)
Offered
Fall Semester
Description
This course is intended to introduce students to basic principles, concepts
and applications of modern physics that are related and useful to biomedical
sciences.
MED104 Introduction to Epidemiology
Course
Coordinator
Paraskevis D., Scientific Collaborator
Instructors
Credits
3
Hours
Lecture : 3
Practical : 0 (Laboratory/Clinic)
Offered
Fall Semester
Description
This course provides an introduction to the skills needed by public health
professionals and clinicians to critically interpret the epidemiologic literature
and be taught with an emphasis on causal inference in epidemiologic
research.
MED105 Biostatistics
Course
Coordinator
Lamnisos D., Associate Professor
Instructors
Giannakou C., Scientific Collaborator
Pelagia I., Scientific Collaborator
Credits
3
Hours
Lecture : 2
Practical : 3 (Laboratory/Clinic)
Offered
Fall Semester
Description
This course is intended to provide an introduction to statistical methods and
reasoning. Students will understand the concept of sampling variation and its
critical role in the construction of confidence intervals and hypothesis testing.
The statistical methods will be applied to simple medical datasets using the
statistical software SPSS and results will be interpreted.

September 2018 School of Medicine, EUC/Student Handbook
… 44
MED106 Anatomy I
Course
Coordinator
Johnson E., Professor
Instructors
Hadjigeorgiou G., Lecturer
Michalinos D., Lecturer
Ntourakis D., Lecturer
Tsamis K., Scientific Collaborator
O’Neil J., Special scientist
Credits
3
Hours
Lecture : 2
Practical : 4 (Laboratory/Clinic)
Offered
Spring Semester
Description
This course aims to familiarize students with the structure of the
musculoskeletal system, as well as the integumentary, endocrine,
hemopoietic and lymphatic systems of the body, and obtain an
understanding of the regional anatomy to describe structures and their
relationships to each other, through the study of Gross, Surface and
Radiological Anatomy. Detailed Gross Anatomy of the human body,
including sectional anatomy, anatomical basis of clinical conditions, living
anatomy and radiologic anatomy will be presented. Students will address
Clinical Correlations of structure and functions of human body and the
anatomical basis for clinical presentations. Surface Anatomy will include the
study of Important bony landmarks of the body with important vessels and
nerves projections. Radiological Anatomy will include identification of normal
anatomical features in commonly used radiographs (plain & contrast),
computerized tomography (CT) scans and MRI.
The course is designed to integrate a 3-dimensional visualization of
structures with function (physiology) and microstructure (histology), and
enable students to use that knowledge to solve problem. All lectures,
laboratories, group discussions, and clinical problems emphasize
integrations of basic science concepts with clinical significance and
applications.

September 2018 School of Medicine, EUC/Student Handbook
… 45
MED107 Histology - Embryology I
Course
Coordinator
Nikoloussi E., Professor
Instructors
Nikas I., Lecturer
Michaelides A., Lecturer
Constantinou Pavlos, Special scientist
Credits
3
Hours
Lecture : 2
Practical : 4 (Laboratory/Clinic)
Offered
Spring Semester
Description
This course is intended to familiarize students with the microstructure
(histology) and evolution (embryology) of the musculoskeletal system, as
well as the integumentary, endocrine, hemopoietic and lymphatic systems of
the body, and obtain an understanding of their regional histology to describe
structures and their relationships to each other. It is designed to acquaint
Medical students with the fundamental terms, concepts, and principles of the
above systems and their cellular population and extracellular matrix
morphological functions and structure and to integrate microstructure tissue
formation (histology) with evolution of human development (embryology) of
the above described systems. It will serve as a connective foundation upon
which, Structure and Function courses as Anatomy-Histology-Embryology-
Physiology and Biochemistry in Medical sciences will be based.
The course is designed to integrate with lectures, laboratories, group
discussions, Computer Assisted Learning (CAL) and clinical case problems,
a microscopical visualization of those systems’ microstructures (in histology)
and their development (in embryology), with structure (anatomy) and
function (physiology) and enable students to use that knowledge to solve
problems in clinical cases.
MED108 Physiology I
Course
Coordinator
Xanthos T., Professor
Instructors
Karpettas N., Lecturer
Paschou L., Scientific Collaborator
Pessach E., Scientific Collaborator
Credits
3
Hours
Lecture : 2
Practical : 4 (Laboratory/Clinic)
Offered
Spring Semester
Description
The course is intended to give the students a broad overview of specific
structures of the human body and their related physiology. The course is
intended to familiarize students with the basic concepts of physiological
procedures and to allow them to proceed to more advanced biomedical and
medical courses

September 2018 School of Medicine, EUC/Student Handbook
… 46
MED109 Medical Biochemistry II
Course
Coordinator
Patrikios I., Professor
Instructors
Dimas C., Scientific Collaborator
Calder P., Professor, Visiting Faculty
Credits
3
Hours
Lecture : 2
Practical : 4 (Laboratory/Clinic)
Offered
Spring Semester
Description
The objective of the course is to familiarize students with the biochemical
pathways and their relationship with the pathophysiology of diseases and the
application of biochemical diagnostic procedures
MED110 Introduction to Genetics
Course
Coordinator
Stephanou A., Professor
Instructors
Politis P., Scientific Collaborator
Credits
3
Hours
Lecture : 2
Practical : 4 (Laboratory/Clinic)
Offered
Spring Semester
Description
This course is intended to give the student a broad overview of basic
principles underlying general and medical genetics. The students will also
gain current knowledge in the clinical context, covering from the genome
structure and function to mutations, screening for inherited disorders. A key
part of the course will be the ability to dissect problem scenarios into its key
features by thinking in an integrated manner and to looking at problems from
different perspectives.
MPR101Clinical Practicum I
Course
Coordinator
Tsioutis C., Lecturer
Instructors
Xanthos T., Professor
Angouridis A, Lecturer
Agapidaki E, Lecturer
Pavli A, Scientific collaborator
Credits
3
Hours
Lecture : 0
Practical : 4 (Laboratory/Clinic)
Offered
Spring Semester
Description
The overall objective is to provide the students with general and safety
information about the hospitals and to identify the medical student roles,
responsibilities and professional and clinical conduct.

September 2018 School of Medicine, EUC/Student Handbook
… 47
Foundations in Medicine Year 2
MED201 Anatomy II
Course
Coordinator
Johnson E., Professor
Hadjigeorgiou G., Lecturer
Instructors
Friehs I., Professor
Ntourakis D., Lecturer
Karpettas N., Lecturer
Michalinos D., Lecturer
O’Neil J., Special scientist
Credits
3
Hours
Lecture : 3
Practical : 4 (Laboratory/Clinic)
Offered
Fall Semester
Description
This course aims to familiarize students with the structure of the major
systems of the body, and obtain an understanding of the regional anatomy to
describe structures and their relationships to each other, through the study of
Gross, Surface and Radiological Anatomy. Detailed Gross Anatomy of the
human body, including sectional anatomy, anatomical basis of clinical
conditions, living anatomy and radiologic anatomy will be presented.
Students will address Clinical Correlations of structure and functions of
human body and the anatomical basis for clinical presentations. Surface
Anatomy will include the study of Important bony landmarks of the body,
important vessels and nerves and projection of the outline of heart, its
borders, surfaces and valves, lungs, their borders, fissures and hila, pleura,
and abdominal and pelvic organs. Radiological Anatomy will include
identification of normal anatomical features in commonly used radiographs
(plain & contrast), computerized tomography (CT) scans and MRI.
The course is designed to integrate a 3-dimensional visualization of
structures with function (physiology and biochemistry), microstructure
(histology), and development (embryology), and enable students to use that
knowledge to solve relevant clinical problems. All lectures, laboratories,
group discussions, and clinical problems emphasize integrations of basic
science concepts with clinical significance and applications.

September 2018 School of Medicine, EUC/Student Handbook
… 48
MED202 Histology - Embryology II
Course
Coordinator
Nikoloussi E., Professor
Instructors
Michaelides A., Lecturer
Nikas I., Lecture
Constantinou Pavlos, Special scientist
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Fall Semester
Description
This course is aiming to acquaint Medical students to a broad and concrete
overview of Histology, i.e. microstructure and Embryology, i.e. evolution of
organs and systems with respect to human tissue organization and
differentiation in embryological/fetal development. It will familiarize them to
the histological microstructure in combination with the structure and function
of the human body major organs and systems as: the Respiratory, the
Cardiovascular, the Gastrointestinal, the Renal and Urinary System, the
Female and the Male Reproductive systems. Teratogenic factors will be
analyzed and discussed as structural and functional causative factors
inducing types of birth defects to the above described organs and systems ,
as well as types of their repair and rehabilitation under clinical procedures.
Clinical Correlations to microstructure and functions of the human’s body
above described major organs and their histological basis of clinical
presentations related to them will be analyzed. Therefore, Medical students
will be acquainted by this course to understand the role of histology and
embryology for accurate diagnosis of diseases. Thus, the course is going to
serve as a connective foundation upon which, Structure and Function
courses as Anatomy-Histology-Embryology-Physiology and Biochemistry in
Medical sciences will be based.
MED203 Physiology II
Course
Coordinator
Xanthos T., Professor
Karpettas N., Lecturer
Instructors
Pantazopoulos I., Scientific Collaborator
Zachariades A., Scientific Collaborator
Ioannou K. , Scientific Collaborator
Paschou S. , Scientific Collaborator
Pessach E. , Scientific Collaborator
Trompoukis P. , Assistant.Professor
Credits
3
Hours
Lecture : 3
Practical : 4 (Laboratory/Clinic)
Offered
Fall Semester
Description
The course is intended to provide a broad and extensive function overview of
the physiology of the systems of the human body. The course is intended to
familiarize students with the physiology of the various systems of the human
body, namely respiratory, cardiovascular, gastrointestinal, renal and
reproductive systems. The purpose of the course is to explain the
physiological basis of systems homeostasis and to introduce basic
mechanisms which are deranged in disease. This will allow students to
proceed to more advanced medical courses such as pathophysiology and
semiology
September 2018 School of Medicine, EUC/Student Handbook
… 49
MED204 Human Nutrition & Metabolism
Course
Coordinator
Patrikios I., Professor
Instructors
Dimas C., Scientific Collaborator
Calder P., Visiting Faculty
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Fall Semester
Description
• The objective of the course is to familiarize the students with the
Molecular bioavailability, metabolism, storage and biosynthesis of micro and
macro molecules and the regulation of their pathways.
• Description of the biochemical basis of inherited disorders with their
associated sequelae of various metabolisms.
• Description of blood and urine metabolites and their importance in
health and disease.
MED205 Family Medicine & Public Health
Course
Coordinator
Agapidaki E., Lecturer
Instructors
Pavli A. ,Scientific Collaborator
Lavranos G., Associate Professor
Credits
3
Hours
Lecture : 4
Practical : 0 (Laboratory/Clinic)
Offered
Fall Semester
Description
This course is intended to give the student a broad overview of Family
Medicine and Public Health. It is designed to acquaint students with the
fundamental terms, concepts, values and principles of the discipline of
Family Medicine and to open the field of Public health and its complexities.
MED206 Neuroscience
Course
Coordinator
Johnson E., Professor
Instructors
Hadjigeorgiou G., Lecturer
Michalinos D., Lecturer
Friehs G., Professor
Zerris V., Professor
Tsamis K., Scientific Collaborator
O’Neil J., Special scientist
Credits
3
Hours
Lecture : 4
Practical : 4 (Laboratory/Clinic)
Offered
Fall Semester
Description
Neuroscience is an integrated course that aims to familiarize students with
the basic concepts about the organization, structure and function of the
human central nervous system and the sensory organs, which emphasizes
the multidisciplinary study of the central nervous system through the study of
Gross and Radiological Anatomy, Histology, Embryology and
Neurophysiology. Detailed Gross Anatomy of the human body, including

September 2018 School of Medicine, EUC/Student Handbook
… 50
sectional anatomy, anatomical basis of clinical conditions, and radiologic
anatomy will be presented. Students will address Clinical Correlations of
structure and functions of human body and the anatomical and
developmental basis for clinical presentations. Radiological Anatomy will
include identification of normal anatomical features in commonly used
radiographs (plain & contrast), computerized tomography (CT) scans and
MRI. The aim is to enable students to apply these fundamental principles
toward understanding nervous system function and dysfunction, toward
clinical problem-solving in relation to disorders that affect the nervous system
and to provide the necessary foundation in neuroscience upon which
students can build for the rest of the training.
The course is designed to integrate a 3-dimensional visualization of
structures (anatomy) with function (physiology) and microstructure
(histology) and development (embryology), and enable students to use that
knowledge to solve clinical problems. All lectures, laboratories, group
discussions, and clinical problems emphasize the integration of basic
science concepts with clinical significance and applications.
MED207 Medical Psychology
Course
Coordinator
Agapidaki E., Lecturer
Instructors
Credits
3
Hours
Lecture : 3
Practical : 0 (Laboratory/Clinic)
Offered
Fall Semester
Description
The objective of the course is to familiarize students with
• The basis of normal human behaviour and its changes.
• The techniques of doctor – patient communication in health and
disease
MED208 Basic Immunology & Microbiology
Course
Coordinator
Petrou M., Scientific Collaborator
Instructors
Patrikios I., Professor
Stephanou A., Professor
Efstratiou A, Adjunct Professor
Credits
3
Hours
Lecture : 4
Practical : 3 (Laboratory/Clinic)
Offered
Fall Semester
Description
The purpose and objectives of this course is the provision of general and
fundamental knowledge in basic microbiology and immunology principles to
medical students so as to prepare them for the more advanced Medical
Microbiology, infectious and autoimmune diseases. In more detail, to
familiarize students with the multiple roles, the structure,
nutritional/environmental requirements and taxonomy of bacterial, fungal,

September 2018 School of Medicine, EUC/Student Handbook
… 51
viral and parasitic agents, their replication/growth, and virulence and how this
leads to the disease. The course should also provide knowledge about
physical and chemical methods of control, and basic laboratory methods of
isolation and identification of the main pathogens.
In immunology, basic topics will be covered such as the description of cells
and organs of the immune system; the innate immune system including
humoral mechanisms: cytokines & complement; an overview of the adaptive
immune system including antigen processing & presentation; the activation
and regulation of innate and adaptive immunity including cellular
mechanisms & receptor, immunization principles and defense mechanisms
of the human host. Hypersensitivity and autoimmunity reactions will be
explained, including tumor immunology and immunodeficiency. The course
will cover also the subject of vaccination and the and new types of vaccines.
The lab covers basic microbiology techniques of cultures, stains isolation
and identification of the most common pathogens.
MED209 Introduction to Clinical Skills
Course
Coordinator
Xanthos T., Professor
Instructors
Ntourakis D., Lecturer
Karpetas N., Lecture
Michalinos A., Lecture
Trompoukis P., Assistant.Professor
Credits
3
Hours
Lecture : 3
Practical : 4 (Laboratory/Clinic)
Offered
Fall Semester
Description
The course purpose is to document and explain how to talk with patient, take
the history from a patient, examine a patient, formulate the findings into
differential diagnoses and rank these in order of probability.

September 2018 School of Medicine, EUC/Student Handbook
… 52
Foundations of Clinical Practice Year 3
MED301 Pathophysiology I
Course
Coordinator
Xanthos T., Professor
Angourides A., Lecturer
Instructors
Rizos E. Adjunct Asst.Professor.
Karpetas N., Lecture
Tsioutis C., Lecturer
Michalinos A., Lecture
Trompoukis P., Assistant.Professor
Constantinou Paschalis, Special scientist
Antoniou S., Scientific Collaborator
Bourantas L., Scientific Collaborator
Margetis N., Scientific Collaborator
Paschou S., Scientific Collaborator
Pessach E., Scientific Collaborator
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Fall Semester
Description
The course is intended tο familiarize the students with the basic
pathophysiological derangements leading to different symptoms and signs.
The objective of this course is to enhance the students’ knowledge regarding
the detailed pathophysiological mechanisms of disease. The course aims at
allowing students to progress to more advanced medical courses such as
Internal Medicine and the various medical specialties. The objective of the
course is to familiarize students with
The pathogenesis of diseases of the different bodily systems, with
consideration of possible mechanisms and underlying metabolic
derangements, and their manifestation of
Clinical Immunology
Rheumatology
Hematological diseases
Gastrointestinal diseases-liver, biliary tract and pancreatic diseases
MED302 Pathology I
Course
Coordinator
Nikas I., Lecturer
Instructors
Michaelides C., Lecturer
Constantinou Pavlos, Special scientist
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Fall Semester
Description
This course is intended to familiarize students with Pathology, also its broad
applications and clinical significance. It is designed to acquaint students with
the study of Disease in multiple levels -e.g. molecular, etiologic,
pathogenetic, morphologic, prognostic- and connect this knowledge with the
other Disease courses of the medical curriculum that run in parallel
(Pathophysiology I, Semiology I, and Pharmacology I). The purpose of this
course is to serve as a bridge between basic science and clinical practice
and use Pathology as a means to understand Disease.

September 2018 School of Medicine, EUC/Student Handbook
… 53
MED303 Pharmacology I
Course
Coordinator
Polissidis A, Scientific collaborator
Instructors
O’Neil J, Special scientist
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Fall Semester
Description
The course is intended το familiarize the students with the basic
pharmacological concepts and provide the basic pharmacology of specific
systems. The objective of this course is to enhance the students’ knowledge
regarding the detailed pharmacological agents needed to treat disease. The
course aims at allowing students to progress to more advanced medical
courses such as Internal Medicine and the various medical specialties. The
objective of the course is to familiarize students with
The pharmacology of the different bodily systems, along with general
principles of pharmacology
Clinical Immunology
Rheumatology
Hematological diseases
Gastrointestinal diseases-liver, biliary tract and pancreatic diseases
MED304 Semiology I
Course
Coordinator
Tsioutis C., Lecturer
Angouridis A., Lecturer
Instructors
Antoniou S., Scientific Collaborator
Bourantas L., Scientific Collaborator
Margetis N., Scientific Collaborator
Paschou S., Scientific Collaborator
Pessach E., Scientific Collaborator
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Fall Semester
Description
The course is intended to familiarize students with the basic components of
history taking and physical examination and to help them identify normal
clinical findings, as well as common signs and symptoms of Rheumatology /
Clinical Immunology, Hematology, Gastrenterology (including liver, biliary
tract and pancreatic diseases), Skin and Reproductive system.
In addition, the course aims to help students develop communicating skills
with their patients and their environment.
Students will learn to apply all necessary steps leading to a complete patient
history, to the development of a medical report and to the diagnostic
approach of a patient.

September 2018 School of Medicine, EUC/Student Handbook
… 54
MED305 General Surgery
Course
Coordinator
Ntourakis D., Lecturer
Instructors
Fries I., Professor
Hadjigeorgiou G., Lecturer
Michalinos A., Lecturer
Trompoukis P., Assistant.Professor
Antoniou S., Scientific Collaborator
Credits
3
Hours
Lecture : 3
Practical : 4 (Laboratory/Clinic)
Offered
Fall Semester
Description
Basic General Surgery is the introductory course to clinical surgery. It is a
13-week course comprised of amphitheater lectures, laboratory skill-stations,
problem based learning modules, simulation training and hospital clinical
training. This course aims to provide a motivating learning environment in
which the students may acquire the surgical knowledge and the technical
skills necessary for their clinical practice.
MED306 Pathophysiology II
Course
Coordinator
Xanthos T., Professor
Angourides A., Lecturer
Instructors
Rizos E., Adjunct Asst.Professor.
Karpetas N., Lecture
Tsioutis C., Lecturer
Michalinos A., Lecture
Trompoukis P., Assistant.Professor
Constantinou Paschalis, Special scientist
Antoniou S., Scientific Collaborator
Bourantas L., Scientific Collaborator
Margetis N., Scientific Collaborator
Paschou S., Scientific Collaborator
Pessach E., Scientific Collaborator
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Spring Semester
Description
The course is intended to familiarize the students with the basic
pathophysiological derangements leading to different symptoms and signs.
The objective of this course is to enhance the students’ knowledge regarding
the detailed pathophysiological mechanisms of disease. The course aims at
allowing students to progress to more advanced medical courses such as
Internal Medicine and the various medical specialties. The objective of the
course is to familiarize students with
The pathogenesis of diseases of the different bodily systems, with
consideration of possible mechanisms and underlying metabolic
derangements, and their manifestation of
Circulatory System,
Respiratory System,
Endocrine and genital pathophysiology,
Urinary Tract diseases

September 2018 School of Medicine, EUC/Student Handbook
… 55
MED307 Medical Microbiology
Course
Coordinator
Petrou M., Scientific Collaborator
Instructors
Efstratiou A, Adjunct Professor
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Spring Semester
Description
The ultimate goal of this course is to get students to understand how
infectious diseases are caused by microbes and how to recognize, prevent
and treat them, so as to prepare them for entry into the clinical curriculum
and to provide students with an introduction to infectious diseases that will
sustain them through their future medical career.
MED308 Pathology II
Course
Coordinator
Nikas I., Lecturer
Instructors
Michaelides C., Lecturer
Constantinou Pavlos, Special scientist
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Spring Semester
Description
This course is intended to continue giving students a broad overview of
Pathology and it is a sequel of Pathology I. Pathology II is designed to help
students understand Disease in multiple levels -e.g. molecular, etiologic,
pathogenetic, morphologic, prognostic- and connect this knowledge with the
other Disease courses of the medical curriculum that run in parallel
(Pathophysiology II, Semiology II, and Pharmacology II).The course aims to
correlate basic with clinical science and to serve as a foundation to support
students develop an integrated approach towards understanding Disease
MED309 Pharmacology II
Course
Coordinator
Polissidis A, Scientific collaborator
Instructors
O’Neil J, Special scientist
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Spring Semester
Description
The course is intended το familiarize the students with the basic
pharmacological concepts and provide the basic pharmacology of specific
systems. The objective of this course is to enhance the students’ knowledge
regarding the detailed pharmacological agents needed to treat disease. The
course aims at allowing students to progress to more advanced medical
courses such as Internal Medicine and the various medical specialties. The
objective of the course is to familiarize students with the pharmacology of
Circulatory System,
Respiratory System,
Endocrine and genital pathophysiology,
Urinary Tract diseases

September 2018 School of Medicine, EUC/Student Handbook
… 56
MED310 Semiology II
Course
Coordinator
Tsioutis C., Lecturer
Angourides A., Lecturer
Instructors
Antoniou S., Scientific Collaborator
Bourantas L., Scientific Collaborator
Margetis N., Scientific Collaborator
Paschou S., Scientific Collaborator
Pessach E., Scientific Collaborator
Credits
3
Hours
Lecture : 3
Practical : 3 (Laboratory/Clinic)
Offered
Spring Semester
Description
The course is intended to familiarize students with the basic components of
history taking and physical examination and to help them identify normal
clinical findings, as well as common signs and symptoms of the Circulatory
System, Respiratory System, Endocrinology, and Urinary tract System.
In addition, the course aims to help students develop communicating skills
with their patients and their environment.
Students will learn to apply all necessary steps leading to a complete patient
history, to the development of a medical report and to the diagnostic
approach of a patient.

September 2018 School of Medicine, EUC/Student Handbook
… 57
Clinical Medicine Core Year 4
MED407 Clinical Training I (Respiratory and Cardiovascular System)
Course
Coordinator
Pantazopoulos I., Scientific Collaborator, respiratory
Karpettas N., Lecturer, cardiovascular
Instructors
Zachariades A., Scientific Collaborator -Resp.
Toumbis M., Scientific Collaborator -Resp.
Chatzis D., Scientific Collaborator -Cardio
Andrikopoulos G. , Scientific Collaborator -Cardio
Credits
6
Hours
Lecture : 4
Practical : 16 (Laboratory/Clinic)
Offered
Fall Semester
Description
The objective of the course is to familiarize students with
• The clinical manifestations, diagnosis, medical and surgical
management and prevention of the diseases of
o The immune, cardiovascular and respiratory system
MED417 Clinical Training II (Digestive System and Hematology)
Course
Coordinator
Margetis N., Scientific Collaborator – GI
Bourantas L., Scientific Collaborator – Hematology
Instructors
Potamitis G.,Scientific Collaborator –GI
Rokkas T., Visiting Faculty -GI
Gerotziafas G., Scientific Collaborator – Hematology
Danilatou V., Scientific Collaborator –Hematology
Credits
6
Hours
Lecture : 4
Practical : 16 (Laboratory/Clinic)
Offered
Fall Semester
Description
The objective of the course is to familiarize students with
• The clinical manifestations, diagnosis, medical and surgical management
and prevention of the diseases of
•The digestive system and the blood and blood forming organs

September 2018 School of Medicine, EUC/Student Handbook
… 58
MED322 Diagnosis By Imaging
Course
Coordinator
Striggaris K., Visiting Faculry
Instructors
Tsitskari M., Scientific Collaborator
Chlapoutaki C., Visiting Faculty
Credits
3
Hours
Lecture : 5
Practical : 2 (Laboratory/Clinic)
Offered
Spring Semester
Description
The objective of the course is to familiarize students with
• The fundamentals of diagnostic image interpretation and clinical indications
for imaging examinations and special procedures
• The principles of protection from ionizing radiation
MED408 Clinical Training III (Infectious Diseases and Clinical Microbiology)
Course
Coordinator
Tsioutis C., Lecturer
Instructors
Petrikkos G., Professor
Zaoutis T, Professor
Tsiodras S., Scientific Collaborator
Pavli A., Scientific Collaborator
Vasilogiannakopoulos A, Scientific Collaborator
Credits
3
Hours
Lecture : 4
Practical : 6 (Laboratory/Clinic)
Offered
Spring Semester
Description
The objective of the course is to familiarize students with
• The clinical manifestations, diagnosis, medical and surgical management
and prevention of the infectious diseases
MED418 Clinical Training IV (Endocrine System, Uro-Nephrological System and Male
Genital Tract)
Course
Coordinator
Paschou S., Scientific Collaborator - Endocrine
Hadjigavriel M., Scientific Collaborator – Nephrology
Protogerou V., Scientific Collaborator - MGT
Instructors
Ioannou I., Scientific Collaborator –Nephrology
Credits
6
Hours
Lecture : 5
Practical : 14 (Laboratory/Clinic)
Offered
Spring Semester
Description
The objective of the course is to familiarize students with
•The clinical manifestations, diagnosis, medical and surgical management
and prevention of the diseases of
•The endocrine and uro-nephrological system and the male genital tract

September 2018 School of Medicine, EUC/Student Handbook
… 59
Clinical Medicine Core Year 5
MED509 Clinical Training V (Musculoskeletal System)
Course
Coordinator
Tsioutis C., Lecturer –Rheumatology
Zibis A., Scientific Collaborator – Orthopaedics
Instructors
Ristanis S., Scientific Collaborator - Orthopaedics
Starantzis K., Scientific Collaborator - Orthopaedics
Credits
6
Hours
Lecture : 4
Practical : 16 (Laboratory/Clinic)
Offered
Fall Semester
Description
The objective of the course is to familiarize students with
•The clinical manifestations, diagnosis, medical and surgical management
and prevention of the diseases of the Musculoskeletal System
MED519 Clinical Training VI (Nervous System and Psychiatry)
Course
Coordinator
Hadjigeorgiou G., Lecturer—Neurosurgery
Soldatos R., Scientific Collaborator - Psychiatry
Instructors
Tsamis K., Scientific Collaborator –Neurology
Grigoriadis N., Scientific Collaborator -Neurology
Credits
6
Hours
Lecture : 6
Practical : 14 (Laboratory/Clinic)
Offered
Fall Semester
Description
The objective of the course is to familiarize students with
• The clinical manifestations, diagnosis, medical and surgical
management and prevention of the diseases of
• The nervous system and of psychiatric disorders
MED428 Clinical Bioethics and Legal Medicine
Course
Coordinator
O'Neil J., Special Scientist
Nicolaides L., Scientific Collaborator
Instructors
Vanezis P., Visiting Faculty
Credits
3
Hours
Lecture : 7
Practical : 0 (Laboratory/Clinic)
Offered
Spring Semester
Description
The objective of the course is to familiarize students with
•The essential values and other elements of the medical profession,
including the principal ethics and legal responsibilities.
•The application of the principles of social justice to professional practice and
the respect to the autonomy, privacy, beliefs and culture of the patient.
•The methods and applications of forensic medicine and medical
jurisprudence

September 2018 School of Medicine, EUC/Student Handbook
… 60
MED510 Clinical Training VII (Pediatrics)
Course
Coordinator
Zaoutis T, Professor
Hadjipanayis A., Assistant Professor
Instructors
Efstathiou L., Scientific Collaborator
Syngelou A., Scientific Collaborator
Credits
6
Hours
Lecture : 4
Practical : 12 (Laboratory/Clinic)
Offered
Spring Semester
Description
The objective of the course is to familiarize students with
•The process of normal growth of children from birth to adolescence and of
growth abnormalities
• The development of the cognitive and mental functions of children
• The clinical manifestations, management and counselling of genetic
disorders
• The clinical manifestations, diagnosis, medical and surgical
management and prevention of the diseases of children
MED520 Clinical Training VIII (Dermatology)
Course
Coordinator
Rigopoulos D., Scientific Collaborator
Instructors
Constantinou Paschalis, Scientific Collaborator
Credits
3
Hours
Lecture : 2
Practical : 6 (Laboratory/Clinic)
Offered
Spring Semester
Description
The objective of the course is to familiarize students with
•The clinical manifestations, diagnosis, medical and surgical management
and prevention of the diseases of
•The skin and dermatological system
MED530 Medical Therapeutics
Course
Coordinator
Angouridis A, Lecturer
Instructors
Tsioutis C, Lecturer
Karpettas N, Lecturer
Daskalopoulos E, Scientific Collaborator
Rizos E, Adjunct Assistant Professor
Katsiki N., Scientific Collaborator
Lampadiari V., Scientific Collaborator
Credits
3
Hours
Lecture : 4
Practical : 1 (Laboratory/Clinic)
Offered
Spring Semester
Description
The objective of the course is to familiarize students with
•The methods of administering medical treatments, the safe prescription of
pharmaceutical agents and the process of pharmacovigilance

September 2018 School of Medicine, EUC/Student Handbook
… 61
Clinical Medicine Core Year 6
MED661 Symptoms and Interpretation of Complementary Examination Procedures
Course
Coordinator
Rizos E, Adjunct Assistant Professor.
Instructors
Credits
3
Hours
Lecture : 3
Practical : 1 (Laboratory/Clinic)
Offered
Fall Semester
Description
The objective of the course is to familiarize students with
• The methods, applications and interpretation of diagnostic techniques
MED611 Professional Traineeship I (Clinical Training IX (Obstetrics and Gynecology )
Course
Coordinator
Trompoukis P., Assistant.Professor
Instructors
Kreatsa M., Scientific Collaborator
Credits
3
Hours
Lecture : 4
Practical : 6 (Laboratory/Clinic)
Offered
Fall Semester
Description
The objective of the course is to familiarize students with
•The concepts and practices of obstetrics, including pregnancy, birth and
puerperium, and contraceptive methods
•The clinical manifestations, diagnosis, medical and surgical management
and prevention of the diseases of the gynaecological system
MED621 Professional Traineeship II (Clinical Training X (Ophthalmology)
Course
Coordinator
Siganos D., Scientific Collaborator
Instructors
Georgiou T., Scientific Collaborator
Boboridis K., Scientific Collaborator
Ntinioti T., Scientific Collaborator
Topouzis F., Scientific Collaborator
Credits
3
Hours
Lecture : 2
Practical : 6 (Laboratory/Clinic)
Offered
Fall Semester
Description
The objective of the course is to familiarize students with
• The clinical manifestations, diagnosis, medical and surgical
management and prevention of the diseases of the ophthalmologic system

September 2018 School of Medicine, EUC/Student Handbook
… 62
MED631 Primary Care
Course
Coordinator
Symeou A., Special scientist
Instructors
Agapidaki E., Lecturer
Pavli A., Scientific Collaborator
Varounis C., Scientific Collaborator
Credits
3
Hours
Lecture : 2
Practical : 8 (Laboratory/Clinic)
Offered
Fall Semester
Description
The objective of the course is to familiarize students with
•The diagnosis, management and prevention of the most common diseases
encountered in primary care
•The special features of the doctor-patient relationship in primary care
•The functions and services provided by primary care
MED612 Professional Traineeship III (Clinical Training XI (Otorhinolaryngology)
Course
Coordinator
TBA
Instructors
TBA
Credits
3
Hours
Lecture : 2
Practical : 6 (Laboratory/Clinic)
Offered
Spring Semester
Description
The objective of the course is to familiarize students with
•The clinical manifestations, diagnosis, medical and surgical management
and prevention of the diseases of the Ear, Nose and Throat
MED622 Professional Traineeship IV (Clinical Training XII (ER, Toxicology, Oncology and
Palliative Care)
Course
Coordinator
Zamboglou N, Professor (Oncology)
Instructors
Credits
6
Hours
Lecture : 4
Practical : 12 (Laboratory/Clinic)
Offered
Spring Semester
Description
The objective of the course is to familiarize students with
•The clinical manifestations, diagnosis, medical and surgical management
and prevention of the neoplastic diseases, including palliative care
•The management of medical emergencies and acute intoxications

September 2018 School of Medicine, EUC/Student Handbook
… 63
Elective Courses (Pre-Clinical and Clinical)
MED216 – Medical Humanities & History
Course
Coordinator
Friehs I., Associate Professor
Instructors
Credits
3
Hours
Lecture : 3
Practical : 0 (Laboratory/Clinic)
Offered
Fall Semester ( Major Elective )
Description
Medical Humanities is concerned with addressing the human side of
medicine and as such draws theoretical, critical and practical insights from
across the social sciences and the arts to explore the meanings attached to
illness, disease, embodiment, disability, health and therapeutic encounters
(from both a professional and patient perspective). It embraces matters of
ethics, aesthetics, history, representation and reflective practice.
History of medicine addresses the changes and developments in Western
medicine from the Ancient Greek world to the modern times. The course will
discuss the varieties of theory and practice of medicine, the understandings
of the body and illness, and the historical contexts in which medicine can be
understood in the pre-modern world, including classical Greek and Roman
society, medieval Islamic and Western cultures, and Renaissance and early
modern periods.
MED604 Research Methodology and Scientific Writing (Free Elective)
Course
Coordinator
Stephanou A., Professor
Instructors
Agapidaki I, Lecturer
Antoniou S, Scientific Collaborator
Credits
3
Hours
Lecture : 3
Practical : 1 (Laboratory/Clinic)
Offered
Fall Semester
Description
This is a basic introductory course in research methodology that will also
include statistical analyses and covers a comprehensive range of topics for
students that will allow them to apply quantitative/qualitative research using
a critical thinking approach. Moreover, examples of clinical trial studies,
protocols and international guidelines for that purposes will also be
discussed. This is a theory-based course along with exercising on research
proposition and with plenty of opportunities to apply the concepts via
practical and interactive activities integrated throughout the course.
MAJOR ELECTIVE (TBA)
Course
Coordinator
Instructors
Credits
3
Hours
Lecture :
Practical : (Laboratory/Clinic)
Offered
Spring Semester
Description

September 2018 School of Medicine, EUC/Student Handbook
… 64
FREE ELECTIVE (TBA)
Course
Coordinator
Instructors
Credits
3
Hours
Lecture :
Practical : (Laboratory/Clinic)
Offered
Spring Semester
Description
