
Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Introduction
Note 1: New terms and codes in these rules are based on the WHO Classification of Tumors of the Digestive System 2010 edition.
Note 2: Ninety-eight percent of colon cancers are adenocarcinoma and adenocarcinoma subtypes.
Note 3: Mixed histologies and specific variants or subtypes of adenocarcinoma other than mucinous/colloid or signet ring cell are
rare. A less common combination is mixed adenoneuroendocrine carcinoma (MANEC) 8244 (previously called
adenocarcinoma and carcinoid). The new terminology was originally proposed for tumors arising from goblet cell carcinoid
but with more aggressive adenocarcinoma histology. It was also proposed because carcinoids are a subgroup of
neuroendocrine carcinoma. Pathologists may still diagnose adenocarcinoma and carcinoid, adenocarcinoid, or
adenocarcinoma and a specific neuroendocrine tumor or adenocarcinoma arising from/with a NET (including specific types
of NET-like goblet cell carcinoid). Over time, the histologic diagnoses will change to MANEC.
Note 4: De novo (previously called frank) adenocarcinoma arises in the mucosa of the bowel, not in a polyp.
Note 5: Terms Seen More Frequently: NET, NEC, GIST
• NET (neuroendocrine tumor): The term NET is gradually replacing carcinoid; however, some pathologists still use the
term carcinoid
• NEC (neuroendocrine carcinoma): The term NEC includes small cell neuroendocrine carcinoma, large cell
neuroendocrine carcinoma, and poorly differentiated neuroendocrine carcinoma
• GIST (gastrointestinal stromal tumor):
o GISTs were originally thought to be smooth muscle tumors but are now thought to originate from the interstitial
cells of Cajal, neuro-regulatory cells in the GI tract. Prior to the implementation of an ICD-O-3 histology code for
GISTs in 2001, they were reported as a GI sarcoma, usually leiomyosarcoma
o GISTs are more common in the stomach (60%) and small intestine (30%), but 1-2% occur in the colon and 3% in
the rectum
o About a quarter of gastric GISTs are malignant
o It is often difficult for the pathologist to determine the behavior of a GIST
o GIST NOS becomes a reportable neoplasm beginning with cases diagnosed 1/1/2021 forward
Note 6: Tables and rules refer to ICD-O rather than ICD-O-3. The version is not specified to allow for updates. Use the currently
approved version of ICD-O.
Note 7: 2007 MPH Rules and 2018 Solid Tumor Rules are used based on date of diagnosis.
• Tumors diagnosed 01/01/2007 through 12/31/2017: Use 2007 MPH Rules
Colon Solid Tumor Rules
September 2021 Update
1

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
• Tumors diagnosed 01/01/2018 and later: Use 2018 Solid Tumor Rules
• The original tumor diagnosed before 1/1/2018 and a subsequent tumor diagnosed 1/1/2018 or later in the same primary
site: Use the 2018 Solid Tumor Rules.
Note 8: For those sites/histologies which have recognized biomarkers, the biomarkers are most frequently used to target treatment.
Currently, there are clinical trials being conducted to determine whether these biomarkers can be used to identify multiple
primaries and/or histologic type. Follow the Multiple Primary Rules; do not code multiple primaries based on biomarkers.
Changes from 2007 MPH Rules
These changes are effective with cases diagnosed 1/1/2018 and later.
1. 2007 Rules instruct “Code the histology from the most representative specimen.” For all sites except breast and CNS, 2018 Rules
instruct “Code the most specific histology from biopsy or resection. When there is a discrepancy between the biopsy and resection
(two distinctly different histologies/different rows), code the histology from the most representative specimen (the greater amount
of tumor).”
2. Rectum and Rectosigmoid are now included with the Colon Rules. In the 2007 MPH Rules, they were included with Other Sites.
3. There are new multiple primary rules which address anastomotic recurrence.
4. Neuroendocrine tumors (formerly carcinoid) arising in the appendix are reportable for cases diagnosed 1/1/2015 and forward.
5. Rule clarification: Pseudomyxoma peritonei (accumulation of mucin-secreting tumor cells in the abdominal or pelvic cavity)
now has a two-tiered system (WHO 2010) that classifies pseudomyxoma peritonei as either high-grade or low-grade (see
below). Pseudomyxoma peritonei is usually associated with mucinous tumors of the appendix and is rarely associated with
ovarian mucinous tumors.
• High-grade pseudomyxoma peritonei is malignant /3
• Low-grade pseudomyxoma peritonei is not malignant /1
• See Histology Rules for coding instructions
Colon Solid Tumor Rules
September 2021 Update
2

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
6. There are dysplasias which have been assigned an in situ behavior code /2 in WHO and in the ICD-O Update. Despite
becoming a /2, they are not reportable in the US. They are reportable in Canada.
• Dysplasia was not collected in the past. If dysplasia is added to the database with the same code as in situ tumors, there
will be a huge upsurge in the incidence of in situ neoplasms. The various agencies are looking for solutions to this
issue.
• There would be no way to separate the dysplasias from the in-situ neoplasms in the database, which would cause
problems with surveillance (long-term studies) since the prognosis and probabilities of disease progression are different
between an in-situ tumor and a dysplasia
• Pathologists frequently use the term “severe dysplasia” or “high grade dysplasia” in place of carcinoma in situ.
Code CIS only if the pathologist expressly states “CIS”
7. Polyps are now disregarded when coding histology. For example, adenocarcinoma in an adenomatous polyp is coded as
adenocarcinoma 8140. For the purposes of determining multiple primaries, tumors coded as adenocarcinoma in a polyp for pre-
2018 cases should be treated as adenocarcinoma 8140.
New codes/terms are identified by asterisks (*) in the histology table in the Terms and Definitions.
New for 2022
1. Timing changes to rules M7 and M8: The timing for subsequent tumors at the anastomosis has changed from 24 months to 36
months. The change is effective for cases diagnosed beginning 1/1/2022 forward. For cases diagnosed 1/1/2018 through
12/31/2021, the timing rule remains at 24 months.
2. Low grade appendiceal neoplasm (LAMN) will become reportable effective for cases diagnosed 1/1/2022 forward. LAMN
may be either in situ 8480/2 or malignant 8480/3 based on physician statement of behavior. LAMN diagnosed prior to
1/1/2022 are not reportable.
Colon Solid Tumor Rules
September 2021 Update
3

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Equivalent or Equal Terms
These terms can be used interchangeably:
• And; with
Note: “And” and “with” are used as synonyms when describing multiple histologies within a single tumor.
• Carcinoid; NET; neuroendocrine tumor
• Carcinoma; adenocarcinoma;
o A histology type must be stated for these terms to be equal
o Example: Mucinous carcinoma and mucinous adenocarcinoma are both coded 8480
• De novo; frank adenocarcinoma (obsolete)
• Familial polyposis; familial adenomatous polyposis (FAP) 8220
• Intramucosal; lateral extension within the mucosal layer of the GI tract
• Invasion through colon wall; extension through colon wall; transmural
Note: The term “transmural” is used to describe extension through all layers of the wall, but not past the wall OR extension through
the serosa into the mesentery. Read the pathology report carefully.
• Mucinous; mucoid; mucous; colloid
• Neuroendocrine carcinoma; NEC
• Polyp; adenoma; polyp NOS; adenomatous polyp
Note 1: The term “polyp” means projecting from a surface.
Note 2: There are many kinds of polyps. Most common are adenomas, which are part of the adenoma-cancer sequence.
Note 3: Other types of polyps include hyperplastic, juvenile, Peutz-Jeghers and serrated adenoma/polyp.
• Serosa; visceral peritoneum
• Simultaneous; existing at the same time; concurrent; prior to first course treatment
• Site; topography
• Tumor; mass; tumor mass; lesion; neoplasm
o
The terms tumor, mass, tumor mass, lesion, and neoplasm are
not
used in a standard manner in clinical diagnoses,
scans, or consults.
Disregard
the terms unless there is a
physician’s statement
that the term is malignant/cancer
o
These terms are used
ONLY
to determine multiple primaries
o
Do not
use these terms for casefinding or determining reportability
• Type; subtype; variant
Colon Solid Tumor Rules
September 2021 Update
4

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Terms that are NOT Equivalent or Equal
These terms are not equivalent. There are no casefinding implications.
• Carcinoma, NOS 8010 is not equivalent to adenocarcinoma, NOS 8140
• Component is not equivalent to subtype/type/variant
Note: Component is only coded when the pathologist specifies the component as a second carcinoma.
• Exophytic and polypoid are not equivalent to either an adenoma or an adenomatous polyp. The terms “exophytic” and
“polypoid” refer to anything projecting from the bowel mucosa into the lumen. The lesion may be benign, malignant, or
inflammatory.
• Phenotype is not equivalent to subtype/type/variant
• Polypoid adenocarcinoma is not equivalent to adenocarcinoma in a polyp
Colon Solid Tumor Rules
September 2021 Update
5

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Table 1: Specific Histologies, NOS, and Subtypes/Variants
Use Table 1 as directed by the Histology Rules to assign the more common histology codes for malignancies found in the colon,
rectosigmoid and rectum.
Note 1: Rare histologies may not be listed in the table. When a histology term is not found, reference ICD-O and all updates.
Note 2: Submit a question to Ask a SEER Registrar when the histology code is not found in Table 1, ICD-O or all updates.
Note 3: Behavior codes are listed when the term has only one possible behavior (either a /2 or /3). For histologies which may be
either /2 or /3, a behavior code is not listed. Code behavior from pathology.
Column 1 contains specific and NOS histology terms.
• Specific histology terms do not have subtypes/variants
• NOS histology terms do have subtypes/variants
Column 2 contains synonyms for the specific or NOS term. Synonyms have the same histology code as the specific or NOS term.
Column 3 contains subtypes/variants of the NOS histology. Subtypes/variants do not have the same histology code as the NOS
term.
Specific and NOS Term and Code
Synonyms for Specific or NOS Term
Subtypes/Variants
Adenocarcinoma 8140
Note 1: See Histology Rules
for
instructions on coding
adenocarcinoma
subtypes/variants arising in a
polyp
Note 2: When the term intestinal
adenocarcinoma is used to
describe a colon primary, it
simply means the appearance is
Adenocarcinoma, NOS
Adenocarcinoma/carcinoma in a polyp
NOS
(now coded to 8140)
Adenocarcinoma/carcinoma in adenomatous
polyp (now coded to 8140)
Adenocarcinoma/carcinoma in polypoid
adenoma (now coded to 8140)
Adenocarcinoma/carcinoma in serrated
adenoma (now coded to 8140)
Adenocarcinoma and mucinous carcinoma,
mucinous documented as less than 50% of
tumor OR percentage of mucinous
Adenoid cystic carcinoma 8200
Cribriform comedo-type carcinoma/
adenocarcinoma, cribriform comedo-type
8201*
Diffuse adenocarcinoma/carcinoma 8145
High grade appendiceal mucinous neoplasm
(HAMN)/Low grade appendiceal mucinous
neoplasm 8480- see Note 3
Linitis plastica 8142/3Medullary
adenocarcinoma/carcinoma 8510
Micropapillary carcinoma 8265*
Mucinous/colloid adenocarcinoma/carcinoma
Colon Solid Tumor Rules
September 2021 Update
6

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Specific and NOS Term and Code
Synonyms for Specific or NOS Term
Subtypes/Variants
similar to adenocarcinoma seen in
the stomach and is coded to
adenocarcinoma NOS 8140
Note 3:Effective 1/1/2022, LAMN
becomes reportable and is coded
8480/2, unless the pathologist
indicates invasive behavior, which
is coded 8480/3. HAMN can be
either /2 or /3 depending on the
pathologist statement of behavior.
unknown/not documented
Adenocarcinoma and signet ring cell carcinoma,
percentage of signet ring cell carcinoma
documented as less than 50% of tumor OR
unknown/not documented
Adenocarcinoma/carcinoma in tubular polyp
(now coded to 8140)
Adenocarcinoma/carcinoma in tubulovillous
polyp (now coded to 8140)
Adenocarcinoma/carcinoma in villous adenoma
(now coded to 8140)
Adenocarcinoma in any type of polyp
Adenocarcinoma, intestinal type
Adenocarcinoma and cribriform carcinoma
percentage of cribriform documented as less
than 50% of tumor OR unknown/not
documented
Adenocarcinoma with mucinous and signet
ring cell features
Comedocarcinoma
Intestinal adenocarcinoma
8480
Mucoepidermoid carcinoma 8430
Serrated adenocarcinoma 8213*
Signet ring cell/poorly cohesive
adenocarcinoma/carcinoma 8490
Superficial spreading adenocarcinoma 8143
Tubulopapillary carcinoma 8263
Undifferentiated adenocarcinoma/carcinoma
8020
Adenosquamous carcinoma 8560
Note: This code cannot be used for
adenocarcinoma subtypes/variants with
squamous cell/epidermoid carcinoma
Mixed adenocarcinoma NOS and epidermoid
carcinoma
Mixed adenocarcinoma NOS and squamous cell
carcinoma
Combined small cell carcinoma 8045
Small cell carcinoma mixed with
• Adenocarcinoma OR
• Neuroendocrine carcinoma OR
• Any other type of carcinoma/adenocarcinoma
Gastrinoma 8153
Colon Solid Tumor Rules
September 2021 Update
7

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Specific and NOS Term and Code
Synonyms for Specific or NOS Term
Subtypes/Variants
Gastrointestinal stromal tumor 8936/3
Note: See standard setter reportability
guidelines.
Gastrointestinal stromal tumor
GIST, NOS
GIST, malignant
Gastrointestinal stromal sarcoma
Mixed adenoneuroendocrine
carcinoma 8244
Adenocarcinoma ex-goblet cell
Adenocarcinoma mixed with high-grade large
cell neuroendocrine carcinoma
Adenocarcinoma mixed with high-grade small
cell neuroendocrine carcinoma
MANEC
Goblet cell adenocarcinoma/Goblet cell
carcinoid 8243
Neuroendocrine carcinoma 8246
NEC
Large cell NEC 8013
Small cell NEC 8041
Neuroendocrine tumor Grade 1 (G1)
8240
Note: When the diagnosis is exactly
“carcinoid” it may be a Grade 1 or
Grade 2 NET. Default is coding
NET Grade 1 8240.
Carcinoid NOS
Low-grade neuroendocrine tumor
NET Grade 1 (G1)
Well differentiated neuroendocrine tumor
EC cell serotonin-producing
NET/enterochromaffin cell carcinoid 8241
Neuroendocrine tumor (NET) Grade 2 (G2) 8249
Somatostatin-producing NET 8156
Sarcoma NOS 8800/3
Angiosarcoma/hemangiosarcoma 9120/3
Leiomyosarcoma 8890/3
Spindle cell carcinoma 8032
Squamous cell carcinoma 8070
Epidermoid carcinoma NOS
Squamous cell carcinoma NOS
Squamous cell epithelioma
*These new codes were approved by the IARC/WHO Committee for ICD-O.
Colon Solid Tumor Rules
September 2021 Update
8

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Table 2: Histologies Not Reportable for Colon, Rectosigmoid and Rectum
Column 1 lists the non-reportable histology term and code for NOS or specific
Column 2 lists the synonym(s) for the term
Column 3 lists the subtype/variant of the NOS term with the histology code
Column 4 lists the reason these histologies are not reportable
Specific or NOS Term and
Code
Synonyms
Subtype/Variant of NOS
with Histology Code
Reason not reportable
Adenoma 8140/0
Note: No malignancy in
polyps
Adenoma NOS
Tubular adenoma 8211/0
Tubulovillous adenoma 8263/0
Villous adenoma 8261/0
Non-malignant
Adenomatous polyp, high
grade dysplasia 8210/2
Non-reportable terminology
Cowden-associated polyp No
code
Note: No malignancy in
polyps
Cowden disease
Cowden syndrome
Multiple hamartoma syndrome
Non-malignant /no code
Dysplasia, high grade 8148/2
Note: Colorectal primaries
only (C180-C189, C199
and C209)
High-grade dysplasia
Intraepithelial neoplasia, high
grade
CURRENTLY NOT REPORTABLE
Dysplasia, low grade 8148/0*
Note: Colorectal primaries
only (C180-C189, C199
and C209)
Intraepithelial neoplasia, low
grade
Non-malignant
Colon Solid Tumor Rules
September 2021 Update
9

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Specific or NOS Term and
Code
Synonyms
Subtype/Variant of NOS
with Histology Code
Reason not reportable
Familial adenomatous
polyposis (FAP) No code
Adenomatous polyposis coli
Bussey-Garder polyposis
Familial multiple polyposis
Familiar polyposis coli
Familial polyposis of the colon
and rectum
Familial polyposis of the
gastrointestinal tract
Gardner syndrome
Multiple adenomatosis
Reportable only when there is cancer in a
polyp
Gangliocytic paraganglioma
8683/0
Non-malignant
Gastrointestinal stromal
tumor stated as benign,
borderline, or non-malignant
8936/1 (SEE NOTE in
column 2)
GIST NOS
GIST, behavior not specified
Note: Gastrointestinal stromal
tumor, NOS is not reportable for
cases diagnosed prior to
1/1/2021. Cases diagnosed
1/1/2021 forward are reportable
Non-malignant
Hyperplastic polyp No code
Non-malignant/no code
Inflammatory or
pseudopolyp No code
Reactive lesions; mimic carcinoma
Intestinal-type adenoma,
high grade 8144/2
Non-reportable terminology
Colon Solid Tumor Rules
September 2021 Update
10

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Specific or NOS Term and
Code
Synonyms
Subtype/Variant of NOS
with Histology Code
Reason not reportable
Juvenile polyp No code
Combined juvenile
polyposis/hereditary
Hemorrhagic telangietasis
(Osler-Webec-Rendu) syndrome
Familial juvenile polyposis
Generalized juvenile polyposis
Hamartomatous gastrointestinal
polyposis;
Juvenile polyposis
Juvenile polyposis coli
Juvenile polyposis of infancy
Non-malignant / no code
L cell glucagon-like peptide
and PP/PYY-producing
NETs 8152/1*
Non-malignant
Leiomyoma 8890/0
Non-malignant
Lipoma 8850/0
Benign accumulation of fat cells that are
circumscribed or encapsulated
Low-grade appendiceal
mucinous neoplasm 8480/1
Note: May have low-grade,
non-invasive
pseudomyxoma
peritonei, mucinous
implants in peritoneum
or beyond
LAMN
Non-malignant
Note: LAMN is non-reportable for cases
diagnosed prior to 1/1/2022. Beginning
1/1/2022, LAMN becomes a reportable
neoplasm- See Table 1
Lynch syndrome No code
Non-malignant/no code
Colon Solid Tumor Rules
September 2021 Update
11

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Specific or NOS Term and
Code
Synonyms
Subtype/Variant of NOS
with Histology Code
Reason not reportable
Mesenchymal tumors
Granular cell tumor 9580/0
Hemangioma 9120/0
Non-malignant
Peutz-Jeghers polyp No code
Intraepithelial neoplasia in
Peutz-Jeghers polyp(s)
Periorificial lentiginosis
Peutz-Jeghers polyposis
Polyps-and-spots syndrome
Non-malignant/no code
Pseudomyxoma peritonei
(when pathologist does not
designate as malignant OR
implants are benign) 8480/1
Non-malignant. When both implants and
site of origin are benign, the case is not
reportable.
Serrated dysplasia, high
grade 8213/2
Non-reportable terminology
Sessile serrated
adenoma/polyp 8213/0*
Note: No malignancy in
polyps
Serrated polyposis
Sporadic serrated polyps
Traditional serrated adenoma
Non-malignant
Tubular adenoma, high
grade 8211/2
Non-reportable terminology
Tubular carcinoid, no
malignancy 8245/1
Non-malignant
Tubulovillous adenoma, high
grade 8263/2
Non-reportable terminology
Villous adenoma, high grade
8261/2
Non-reportable terminology
*These new codes were approved by the IARC/WHO Committee for ICD-O
Colon Solid Tumor Rules
September 2021 Update
12

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Illustrations
Colonoscopy measurements which may be used to determine primary site when no site is designated
Colon Solid Tumor Rules
September 2021 Update
13


Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
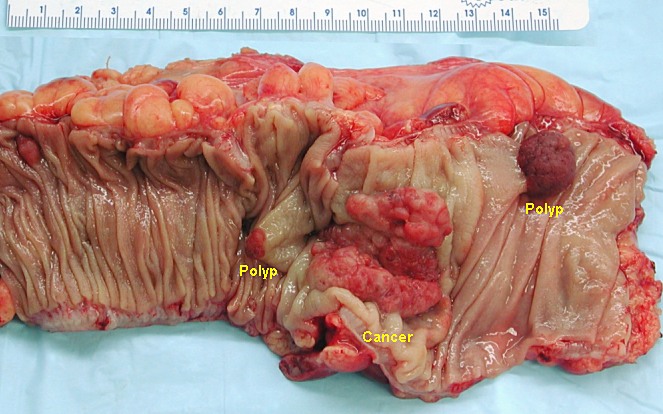
Polyps and de novo or “frank” adenocarcinoma in colon
Source: http://upload.wikimedia.org/wikipedia/commons/4/44/Colon_cancer.jpg
Colon Solid Tumor Rules
September 2021 Update
15

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Large intestine; snare instrument to remove polyps
Colon Solid Tumor Rules
September 2021 Update
16

Colon, Rectosigmoid, and Rectum Equivalent Terms and Definitions
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Multiple Primary Rules
Jump to Histology Coding Rules
Colon Surgery: Hemicolectomy
The primary treatment for colon cancer is surgery. Part of the large bowel and the surrounding lymph nodes are removed. The
remaining bowel is then joined together (anastomosis).
http://www.cedars-sinai.edu/Patients/Programs-and-Services/Colorectal-Cancer-Center/Services-and-Treatments/Rectal-Cancer.aspx
Colon Solid Tumor Rules
September 2021 Update
17



Colon, Rectosigmoid, and Rectum Multiple Primary Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Histology Coding Rules
Note 1: These rules are NOT used for tumor(s) described as metastases. Metastatic tumors include but are not limited to:
• Discontinuous lesions in soft tissue adjacent to
primary site
• Regional or distant lymph nodes for the
primary site being abstracted as identified in
Summary Staging Manual
• Brain
• Liver
• Lung
• Peritoneum
• Spinal cord (not frequent)
Note 2: 2007 MPH Rules and 2018 Solid Tumor Rules are used based on date of diagnosis.
• Tumors diagnosed 01/01/2007 through 12/31/2017: Use 2007 MPH Rules
• Tumors diagnosed 01/01/2018 and later: Use 2018 Solid Tumor Rules
• The original tumor diagnosed before 1/1/2018 and a subsequent tumor diagnosed 1/1/2018 or later in the same
primary site: Use the 2018 Solid Tumor Rules
Unknown if Single or Multiple Tumors
Note: Collision tumors are counted as two individual tumors for the purpose of determining multiple primaries. Collision tumors
were originally two separate tumors that arose in close proximity. As the tumors increased in size, they merged or overlapped
each other. Use the Multiple Tumors module.
Rule M1 Abstract a single primary
i
when it is not possible to determine if there is a single tumor or multiple tumors.
Note 1: Use this rule only after all information sources have been exhausted.
Note 2: Examples of cases with minimal information include
• Death certificate only (DCO)
• Cases for which information is limited to pathology report only
ο Outpatient biopsy with no follow-up information available
ο Multiple pathology reports which do not specify whether a single tumor or multiple tumors have been biopsied
and/or resected
This is the end of instructions for Unknown if Single or Multiple Tumors
i
Prepare one abstract. Use the histology rules to assign the appropriate histology code.
Colon Solid Tumor Rules
September 2021 Update
20

Colon, Rectosigmoid, and Rectum Multiple Primary Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Histology Coding Rules
Single Tumor
Note: Collision tumors are counted as two individual tumors for the purpose of determining multiple primaries. Collision tumors
were originally two separate tumors that arose in close proximity. As the tumors increased in size, they merged or overlapped
each other. Use the Multiple Tumors module.
Rule M2 Abstract a single primary
i
when there is a single tumor.
Note 1: A single tumor is always a single primary.
Note 2: The tumor may overlap onto or extend into adjacent/contiguous site or subsites.
Note 3: The tumor may have in situ and invasive components.
Note 4: The tumor may have two or more histologic components.
This is the end of instructions for Single Tumor
i
Prepare one abstract. Use the histology rules to assign the appropriate histology code.
Colon Solid Tumor Rules
September 2021 Update
21

Colon, Rectosigmoid, and Rectum Multiple Primary Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Histology Coding Rules
Multiple Tumors
Note 1: Multiple tumors may be a single primary or multiple primaries.
Note 2: Collision tumors are counted as two individual tumors for the purpose of determining multiple primaries. Collision tumors
were originally two separate tumors that arose in close proximity. As the tumors increased in size, they merged or overlapped
each other. Use the Multiple Tumors module to determine if they are a single primary or multiple primaries.
Rule M3 Abstract a single primary
i
when there is adenocarcinoma in situ and/or invasive in at least one polyp AND
• There is a clinical diagnosis of familial polyposis (FAP) OR
• Greater than 100 polyps are documented (no diagnosis of FAP)
Note 1: A diagnosis of familial polyposis (FAP) is made when the patient has greater than 100 adenomatous polyps. Polyps with
adenocarcinoma and benign polyps will be present. Because there are many polyps, the pathologist does not examine every
polyp.
Note 2: In situ /2 and malignant /3 adenocarcinoma in polyps, malignancies with remnants of a polyp, as well as de novo
(previously called frank) malignancies may be present in multiple segments of the colon or in both the colon and rectum.
Polyposis may be present in other GI sites such as stomach (a de novo does not have to be present; all adenocarcinoma
may be in polyps).
Note 3: FAP is a genetic disease. The characteristics of FAP are numerous precancerous polyps in the colon and rectum when
the patient reaches puberty. If not treated, the polyps typically become malignant. Patients often have total colectomies.
Note 4: Multiple polyps in the colorectum is not equivalent to FAP.
Note 5: Code primary site as follows:
• Present in more than one segment of colon: C189 colon, NOS
• Present in colon and rectosigmoid OR colon and rectum: C199 rectosigmoid junction
• Present in colon and small intestine: C260 intestinal tract, NOS (there is no code for large and small bowel)
Note: In addition to the colon and small intestine, FAP may also be present in the:
• Stomach AND/OR
• Rectosigmoid AND/OR
• Rectum
Example: The patient has a diagnosis of FAP. The operative report and physician’s documentation say that polyps with
adenocarcinoma were present in specimens removed from the ascending colon and the sigmoid colon. The
ascending and sigmoid colon are part of the large bowel. Code the primary site C189 colon NOS.
Colon Solid Tumor Rules
September 2021 Update
22
Colon, Rectosigmoid, and Rectum Multiple Primary Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Histology Coding Rules
Rule M4 Abstract multiple primaries
ii
when there are separate, non-contiguous tumors in sites with ICD-O site codes that differ
at the second CXxx and/or third CxXx character.
Note 1: Definition of separate/non-contiguous tumors: at least two malignancies which do not overlap/merge.
Note 2: Differences at either the second or third characters are different primary sites/multiple primaries.
Example 1: Breast C50x and colon C18x
Example 2: Colon C18x and rectum C209 (This does not include FAP- see earlier rules)
Note: This rule does not apply to a single overlapping malignancy of colon and rectum.
Rule M5 Abstract multiple primaries
ii
when separate/non-contiguous tumors are two or more different subtypes/variants in
Column 3, Table 1 in the Equivalent Terms and Definitions. Timing is irrelevant.
Note: The tumors may be subtypes/variants of the same or different NOS histologies.
• Same NOS: Medullary carcinoma NOS 8510/3 and tubulopapillary adenocarcinoma 8263/3 are both subtypes of
adenocarcinoma NOS 8140/3 but are distinctly different histologies. Abstract multiple primaries.
• Different NOS: Goblet cell carcinoid 8243/3 is a subtype of mixed adenoneuroendocrine carcinoma 8244/3;
somatostatin-producing NET 8156/3 is a subtype of neuroendocrine tumor Grade 1 (G1) 8240/3. They are distinctly
different histologies. Abstract multiple primaries.
Rule M6 Abstract multiple primaries
ii
when separate/non-contiguous tumors are on different rows in Table 1 in the Equivalent
Terms and Definitions. Timing is irrelevant.
Note: Each row in the table is a distinctly different histology.
Rule M7 Abstract multiple primaries
ii
when a subsequent tumor arises at the anastomotic site AND:
• One tumor is a NOS and the other is a subtype/variant of that NOS OR
• The subsequent tumor occurs greater than 36 months after original tumor resection OR
Note: For cases diagnosed prior to 1/1/2022, the time interval is greater than 24 months.
• The subsequent tumor arises in the mucosa (see illustration)
Note: Bullet three does not apply to GIST. GISTs only start in the wall; never in the mucosa.
Example: (For bullet 1: NOS and subtype/variant) The original tumor was adenocarcinoma NOS 8140. The patient had a
hemicolectomy. There was a recurrence at the anastomotic site diagnosed exactly as mucinous adenocarcinoma 8480.
Mucinous adenocarcinoma is a subtype/variant of the NOS adenocarcinoma, but they are two different histologies. Code
two primaries, one for the original adenocarcinoma NOS and another for the subsequent anastomotic site mucinous
adenocarcinoma.
Note 1: There may or may not be physician documentation of anastomotic recurrence. Follow the rules.
Colon Solid Tumor Rules
September 2021 Update
23

Colon, Rectosigmoid, and Rectum Multiple Primary Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Histology Coding Rules
Note 2: When the original tumor was diagnosed prior to 1/1/2018 and was coded to adenocarcinoma in a polyp, and the
anastomotic site tumor is adenocarcinoma per 2018 rules, the tumors are the same histology. ICD-O codes differ because
of changes in histology coding rules.
Note 3: The tumor may or may not invade into the colon wall or adjacent tissue.
Note 4: A “rectal stump” is an anastomotic site.
Note 5: These rules are hierarchical. Only use this rule when previous rules do not apply.
Rule M8 Abstract a single primary
i
when a subsequent tumor arises at the anastomotic site AND:
• The subsequent tumor occurs less than or equal to 36 months after original tumor resection OR
Note: For cases diagnosed prior to 1/1/2022, timing is less than or equal to 24 months
• The tumor arises in colon/rectal wall and/or surrounding tissue; there is no involvement of the mucosa (see
illustration) OR
• The pathologist or clinician documents an anastomotic recurrence
Note 1: Bullet two does not apply to GIST. GISTs only start in the wall; never in the mucosa.
Note 2: The physician may stage the subsequent tumor because the depth of invasion determines the second course of treatment.
Note 3: These tumors are a single primary/recurrence. Registrars that collect recurrence information should record the
information in the recurrence fields.
Note 4: A “rectal stump” is an anastomotic site.
Rule M9 Abstract multiple primaries
ii
when there are separate, non-contiguous tumors in sites with ICD-O site codes that differ
at the fourth characters C18X.
Note: Differences at the fourth character include different segments of the colon. Abstract a primary for each separate non-
contiguous tumor in a different segment of the colon. This rule is not used for colon NOS C189. C189 is rarely used other
than DCO.
Example: The patient has adenocarcinoma in situ in a sigmoid polyp and mucinous adenocarcinoma in a polyp in the descending
colon, the site code differs at the fourth character (sigmoid C187 and descending C186). Code two primaries, one for
the sigmoid and another for the descending colon.
Colon Solid Tumor Rules
September 2021 Update
24

Colon, Rectosigmoid, and Rectum Multiple Primary Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Histology Coding Rules
Rule M10 Abstract multiple primaries
ii
when the patient has a subsequent tumor after being clinically disease-free for greater
than one year after the original diagnosis or last recurrence.
Note 1: Clinically disease-free means that there was no evidence of recurrence on follow-up.
• Colonoscopies are NED
• Scans are NED
Note 2: When there is a recurrence less than or equal to one year of diagnosis, the “clock” starts over. The time interval is
calculated from the date of last recurrence. In other words, the patient must have been disease-free for greater than one
year from the date of the last recurrence.
Note 3: When the first course of treatment was a polypectomy only, this rule means there were no recurrences for greater than
one year.
Note 4: When the first course of treatment was a colectomy or A&P resection, there were no anastomotic recurrences for
greater than one year.
Note 5: When it is unknown/not documented whether the patient had a recurrence, default to date of diagnosis to compute the
time interval.
Note 6: The physician may state this is a recurrence, meaning the patient had a previous colon tumor and now has another colon
tumor. Follow the rules; do not attempt to interpret the physician’s statement.
Rule M11 Abstract a single primary
i
when synchronous, separate/non-contiguous tumors are on the same row in Table 1 in the
Equivalent Terms and Definitions.
Note: The same row means the tumors are:
• The same histology (same four-digit ICD-O code) OR
• One is the preferred term (column 1) and the other is a synonym for the preferred term (column 2) OR
• A NOS (column 1/column 2) and the other is a subtype/variant of that NOS (column 3)
Rule M12 Abstract a single primary
i
(the invasive) when an in situ tumor is diagnosed after an invasive tumor.
Note 1: The rules are hierarchical. Only use this rule when none of the previous rules apply.
Note 2: The tumors may be a NOS and a subtype/variant of that NOS. See Table 1
in the Equivalent Terms and Definitions for
listings of NOS and subtype/variants.
Note 3: The in situ is recorded as a recurrence for those registrars who collect recurrence data.
Colon Solid Tumor Rules
September 2021 Update
25

Colon, Rectosigmoid, and Rectum Multiple Primary Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Histology Coding Rules
Rule M13 Abstract a single primary
i
(the invasive) when an invasive tumor is diagnosed less than or equal to 60 days after an in
situ tumor.
Note 1: The rules are hierarchical. Only use this rule when previous rules do not apply.
Note 2: Change behavior code on original abstract from /2 to /3. Do not change date of diagnosis.
Note 3: If the case has already been submitted to the central registry, report all changes.
Note 4: The physician may stage both tumors because staging and determining multiple primaries are done for different reasons.
Staging determines which treatment would be most effective. Determining multiple primaries is done to stabilize the data
for the study of epidemiology (long-term studies done on incidence, mortality, and causation of a disease with the goal of
reducing or eliminating that disease).
Note 5: See the COC and SEER manuals for instructions on coding data items such as Date of Diagnosis, Accession Year and
Sequence Number.
Rule M14 Abstract multiple primaries
ii
when an invasive tumor occurs more than 60 days after an in situ tumor.
Note 1: Abstract both the invasive and in situ tumors.
Note 2: Abstract as multiple primaries even if physician states the invasive tumor is disease recurrence or progression.
This rule is based on long-term epidemiologic studies of recurrence intervals. The specialty medical experts (SMEs)
reviewed and approved these rules. Many of the SMEs were authors, co-authors, or editors of the AJCC Staging Manual.
Rule M15 Abstract a single primary
i
when tumors do not meet any of the above criteria.
Note: Use caution when applying this default rule. Please confirm that you have not overlooked an applicable rule.
Example: The pathology states adenocarcinoma in situ 8140/2 and a second non-contiguous invasive adenocarcinoma 8140/3 in the
sigmoid colon C187. Multiple tumors that are the same histology in the same primary site (same four characters of ICD-
O topography code) are a single primary.
This is the end of instructions for Multiple Tumors.
i
Prepare one abstract. Use the histology rules to assign the appropriate histology code. For registries collecting recurrence data: When a
subsequent tumor is “single primary,” record that subsequent tumor as a recurrence.
ii
Prepare two or more abstracts. Use the histology rules to assign the appropriate histology code to each case abstracted.
Colon Solid Tumor Rules
September 2021 Update
26

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
Priority Order for Using Documentation to Identify Histology
IMPORTANT NOTES
1. Code the histology diagnosed prior to neoadjuvant treatment.
Note 1: Histology changes may occur following immunotherapy, chemotherapy, targeted therapy, and radiation therapy.
Note 2: Neoadjuvant treatment is any tumor-related treatment given prior to surgical removal of the malignancy.
Exception: If the initial diagnosis is based on histology from FNA, smears, cytology, or from a regional or metastatic site, and
neoadjuvant treatment is given and followed by resection of primary site which identifies a different or specific histology, code the
histology from the primary site.
2. Code the histology using the following priority list and the Histology Rules. Do not change histology in order to make the case
applicable to staging.
The priority list is used for single primaries (including multiple tumors abstracted as a single primary).
This is a hierarchical list of source documentation.
Code the most specific pathology/tissue from either resection or biopsy.
Note 1: The term “most specific” usually refers to a subtype/variant.
Note 2: The histology rules instruct to code the invasive histology when there are in situ and invasive components in a single tumor.
Note 3: When there is a discrepancy between the biopsy and resection (two distinctly different histologies/different rows), code the histology
from the most representative specimen (the greater amount of tumor).
1. Tissue or pathology report from primary site (in priority order)
A. Addendum(s) and/or comment(s)
B. Final diagnosis / synoptic report as required by CAP
C. CAP protocol
Note 1: Addendums and comments on the pathology report are given a high priority because they often contain information about molecular
testing, genetic testing, and/or special stains which give a more specific diagnosis.
Note 2: The pathologist’s diagnosis from the pathology report is always reliable, so the final diagnosis is the second priority.
Note 3: The CAP protocol is a checklist which:
Colon Solid Tumor Rules
September 2021 Update
27

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
• Provides guidelines for collecting the essential data elements for complete reporting of malignant tumors and optimal patient
care
• Allows physicians to check multiple histologies
2. Tissue/pathology from a metastatic site
Note 1: Code the behavior /3.
Note 2: The tissue from a metastatic site often shows variations from the primary tumor. When it is the only tissue available, it is more
accurate than a scan.
3. Scan: The following list is in priority order.
A. CT
B. PET
C. MRI
4. Code the histology documented by the physician when none of the above are available. Use the documentation in the following
priority order:
A. Treatment plan
B. Documentation from Tumor Board
C. Documentation in the medical record that refers to original pathology, cytology, or scan(s)
D. Physician’s reference to type of cancer (histology) in the medical record
Note 1: Code the specific histology when documented.
Note 2: Code the histology to 8000 (cancer/malignant neoplasm, NOS) or as stated by the physician when nothing more specific is
documented.
5. Cytology (seldom used for colon, rectosigmoid and rectum)
Colon Solid Tumor Rules
September 2021 Update
28

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
Coding Histology
Note 1: The priority is to code the most specific histology. DO NOT USE BREAST HISTOLOGY CODING RULES FOR THIS
SITE.
Note 2: Only use this section for one or more histologies within a single tumor.
Note 3: Do not use this section in place of the Histology Rules.
1. Code the most specific histology or subtype/type/variant, regardless of whether it is described as:
A. The majority or predominant part of tumor
B. The minority of tumor
C. A component
Note 1: Mucinous and signet ring cell carcinoma must meet a percentage requirement in order to be coded. Refer to the Histology Rules if
mucinous and/or signet ring cell carcinoma is present.
Note 2: The terms above (A, B, C) must describe a carcinoma or sarcoma in order to code a histology described by those terms.
Example: When the diagnosis is adenocarcinoma with a component of medullary carcinoma, code medullary carcinoma 8510.
Negative Example: When the diagnosis is simply adenocarcinoma with a medullary component, code adenocarcinoma NOS 8140.
Do not assume this is a medullary carcinoma. This could be medullary differentiation or features.
Note 3: When the most specific histology is described as differentiation or features, see #2.
Example 1: Diagnosis for a single tumor is adenocarcinoma 8140 with the majority or predominant part of tumor being medullary
adenocarcinoma 8510. Code the subtype/variant: medullary adenocarcinoma 8510.
Example 2: Diagnosis for a single tumor is mixed neuroendocrine carcinoma 8244 with minority of tumor being goblet cell carcinoid 8243.
Code the subtype/variant: goblet cell carcinoid 8243.
Example 3: Diagnosis for a single tumor is sarcoma NOS 8800/3 with a component of leiomyosarcoma 8890/3. Code the subtype/variant:
leiomyosarcoma 8890/3.
2. Code the histology described as differentiation or features/features of ONLY when there is a specific ICD-O code for the “NOS
with ____ features” or “NOS with ____ differentiation”.
Note: Do not code differentiation or features when there is no specific ICD-O code.
3. Code the specific histology described by ambiguous terminology (list follows) ONLY when A or B is true:
A. The only diagnosis available is one histology term described by ambiguous terminology
• CoC and SEER require reporting of cases diagnosed only by ambiguous terminology
Colon Solid Tumor Rules
September 2021 Update
29

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
• Case is accessioned (added to your database) based on ambiguous terminology and no other histology information is
available/documented
Example: Outpatient biopsy says probably malignant GIST. The case is accessioned (entered into the database) as required by
both SEER and COC. No further information is available. Code the histology malignant GIST. The case meets the
criteria in #3A.
B. There is a NOS histology and a more specific (subtype/variant) described by ambiguous terminology
• Specific histology is clinically confirmed by a physician (attending, pathologist, oncologist, etc.) OR
• Patient is receiving treatment based on the specific histology described by ambiguous term
Example 1: The pathology diagnosis is adenocarcinoma consistent with micropapillary carcinoma. The oncology consult
says the patient has micropapillary carcinoma of the cecum. This is clinical confirmation of the diagnosis, code
micropapillary carcinoma. The case meets the criteria in bullet 1.
Example 2: The pathology diagnosis is mixed neuroendocrine carcinoma consistent with goblet cell carcinoid. The treatment
plan says the patient will receive the following treatment for goblet cell carcinoid. Treatment plan confirms
goblet cell carcinoid; code goblet cell carcinoid. The case meets the criteria in bullet 2.
If the specific histology does not meet the criteria in #3B, then code the NOS histology.
List of Ambiguous Terminology
Apparently
Appears
Comparable with
Compatible with
Consistent with
Favor(s)
Malignant appearing
Most likely
Presumed
Probable
Suspect(ed)
Suspicious (for)
Typical (of)
Colon Solid Tumor Rules
September 2021 Update
30

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
4. Do not code histology when described as:
• Architecture
• Foci; focus; focal
• Pattern
Colon Solid Tumor Rules
September 2021 Update
31

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
Single Tumor
Rule H1 Code adenocarcinoma with neuroendocrine differentiation 8574 when the final diagnosis is exactly “adenocarcinoma
with neuroendocrine differentiation”.
Note: Do not use this code when:
• The diagnosis is any subtype/variant of adenocarcinoma with neuroendocrine differentiation
• Any modifier other than differentiation is used, i.e., adenocarcinoma with neuroendocrine features
Rule H2 Code the histology and ignore the polyp when a carcinoma originates in a polyp.
Note 1: This is a change from the 2007 MPH rules which instructed registrars to use the codes for malignancies in a polyp, such as
adenocarcinoma in a polyp 8210.
Note 2: Sufficient data has been collected to:
• Determine the frequency with which carcinomas arise within polyps
• Establish patient care guidelines for individuals with colon polyps
Example: Colonoscopy with polypectomy finds mucinous adenocarcinoma in the polyp. Code mucinous adenocarcinoma 8480.
Rule H3 Code combined small cell carcinoma 8045 when the final diagnosis is small cell carcinoma AND any other carcinoma.
Examples:
• Small cell carcinoma 8041 and adenocarcinoma 8140
• Small cell carcinoma 8041 and neuroendocrine carcinoma 8246
Colon Solid Tumor Rules
September 2021 Update
32

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
Rule H4 Code mixed mucinous and signet ring cell as follows:
• Adenocarcinoma with mucinous and signet ring features – code adenocarcinoma 8140
• Mucinous carcinoma and signet ring cell carcinoma:
ο Mucinous carcinoma documented as greater than 50% – code mucinous carcinoma 8480
ο Signet ring cell carcinoma documented as greater than 50% – code signet ring cell carcinoma 8490
ο Percentage of mucinous carcinoma and signet ring cell carcinoma unknown/not designated- code
adenocarcinoma mixed subtypes 8255
Note: This rule is for mucinous carcinoma and signet ring cell carcinoma in a single tumor. For mucinous
adenocarcinoma mixed with another histology OR signet ring cell carcinoma mixed with another histology,
proceed through the rules.
Rule H5 Code low grade appendiceal mucinous neoplasm (LAMN) and high grade appendiceal mucinous neoplasm
(HAMN) 8480/2 when:
• Diagnosis date is 1/1/2022 forward AND
• Behavior is stated to be in situ/non-invasive OR
• Behavior is not indicated
Note 1: ICD-O-3.2 lists LAMN with behavior of /1. WHO 5
th
Ed Digestive Systems Tumors indicates this neoplasm is considered
in situ. After consulting with WHO Digestive System editors, College of American pathologists, and AJCC GI chapter
experts, the standard setting organizations have agreed LAMN should be collected and should be assigned a behavior code
of /2 beginning with cases diagnosed 1/1/2022 forward.
Note 2: A diagnosis of LAMN or HAMN does not require the tumor be comprised of greater than 50% mucinous in order to be
coded 8480.
Note 3: If the pathologist indicates LAMN or HAMN is invasive or has a malignant behavior, continue through the rules.
Rule H6 Code invasive mucinous adenocarcinoma 8480 when the diagnosis is any of the following:
• Exactly “mucinous adenocarcinoma” (no modifiers)
• High grade appendiceal mucinous neoplasm (HAMN) stated to be invasive (DX 1/1/2022 forward)
• High-grade pseudomyxoma peritonei
• Invasive pseudomyxoma peritonei
• Low grade appendiceal mucinous neoplasm (LAMN) stated to be invasive (DX 1/1/2022 forward)
• Malignant pseudomyxoma peritonei
Colon Solid Tumor Rules
September 2021 Update
33

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
• Two histologies and mucinous is documented to be greater than 50% of the tumor
ο Mucinous carcinoma must meet a percentage requirement in order to be coded. Do not use majority of tumor,
predominantly, or predominant part of the tumor to code mucinous 8480.
Note 1: Be very careful when determining primary site; almost all pseudomyxoma peritonei originate in the appendix C181.
However, it can be metastatic disease from sites such as bowel, ovary, or bladder. Code the primary site as designated by
a physician. When the primary site is not designated, code unknown primary C809 and the histology as mucinous
carcinoma 8480.
Note 2: Report the appendiceal mucinous neoplasm as malignant /3 using the ICD-O matrix principle and the SEER and COC
Manuals when the pathology from the appendix is low-grade mucinous neoplasm (not reportable prior to 1/1/2022) AND
• The pseudomyxoma peritonei are high-grade/invasive/malignant OR
• Patient is treated for malignant pseudomyxoma peritonei OR
• The diagnosis is low grade appendiceal mucinous neoplasm (LAMN) and the physician states it is malignant OR
• The diagnosis is high grade appendiceal mucinous neoplasm (HAMN) and the physician states it is
malignant
Note 3: The following are non-reportable for cases diagnosed prior to 1/1/2022:
• Appendiceal neoplasm with low-grade pseudomyxoma peritonei AND no treatment
• No designation of high- or low-grade for the appendiceal neoplasm AND no treatment for the pseudomyxoma
peritonei
Rule H7 Code invasive signet ring cell adenocarcinoma 8490 when the diagnosis is any of the following:
• Exactly signet ring cell carcinoma (no modifiers)
• Adenocarcinoma and signet ring cell carcinoma, where signet ring cell is documented to be greater than 50% of
the tumor
ο Signet ring cell adenocarcinoma must meet a percentage requirement in order to be coded. Do not use majority of
tumor, predominantly, or predominant part of tumor to code signet ring cell 8490.
Rule H8 Code adenocarcinoma NOS 8140 when the final diagnosis is:
• Two histologies:
ο Adenocarcinoma and mucinous carcinoma
• Percentage of mucinous unknown/not documented
• Mucinous documented as less than or equal to 50% of tumor
Colon Solid Tumor Rules
September 2021 Update
34

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
ο Adenocarcinoma and signet ring cell carcinoma
• Percentage of signet ring unknown/not documented
• Signet ring cell documented as less than or equal to 50% of tumor
• Exactly adenocarcinoma OR
• Intestinal type adenocarcinoma OR adenocarcinoma intestinal type (no modifiers or additional histologic terms).
Note 1: Code 8140 adenocarcinoma NOS even if pathology says intestinal type adenocarcinoma.
Note 2: Do not use code 8144 adenocarcinoma intestinal type for colorectal primaries. Intestinal type adenocarcinoma 8144 is
used for tumors which occur in the stomach, head and neck, and specific GYN sites. It is called intestinal because it
resembles carcinoma which occurs in the colon, rectosigmoid or rectum.
Note 3: When a diagnosis of intestinal type adenocarcinoma is further described by a specific term (such as mucinous
intestinal type adenocarcinoma or signet ring cell intestinal type adenocarcinoma), it would be treated as an
adenocarcinoma with a subtype/variant.
Rule H9 Code the histology when only one histology is present.
Note 1: Use Table 1 to code histology. New codes, terms, and synonyms are included in Table 1 and coding errors may occur if
the table is not used.
Note 2: Use the ICD-O and all updates when the histology is not listed in Table 1.
Note 3: Submit a question to Ask a SEER Registrar
when the histology code is not found in Table 1, ICD-O or all updates.
Colon Solid Tumor Rules
September 2021 Update
35

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
Rule H10 Code the invasive histology when in situ and invasive histologies are present in the same tumor.
Rule H11 Code the subtype/variant when there is a NOS and a single subtype/variant of that NOS such as the following:
• Adenocarcinoma 8140 and a subtype/variant of adenocarcinoma
• Mixed adenoneuroendocrine carcinoma 8244 and a subtype/variant of mixed adenoneuroendocrine carcinoma
• Neuroendocrine carcinoma 8246 and a subtype/variant of neuroendocrine carcinoma
• Neuroendocrine tumor Grade 1 (G1) 8240 and a subtype/variant of neuroendocrine tumor Grade 1 (G1)
• Sarcoma 8800 and a subtype/variant of sarcoma
Note 1: See Table 1 in the Equivalent Terms and Definitions to find NOS and subtypes/variants.
Note 2: Only code subtypes/variant when pathology gives an exact diagnosis. Do not code the subtype/variant when modified by
terms such as differentiation, features of, etc., unless there is a specific code for the histology term with the modifier.
This is the end of instructions for Single Tumor.
Code the histology using the rule that fits the case.
Multiple Tumors Abstracted as a Single Primary
Note: Multiple tumors must be a single primary to use this module. See the Multiple Primary Rules
to determine whether these tumors are a
single primary.
Rule H12 Code adenocarcinoma in familial adenomatous polyposis coli (FAP) 8220 when clinical history says the patient has
familial polyposis AND
• The final diagnosis on the pathology report from resection is adenocarcinoma in FAP OR
• There are greater than 100 polyps identified in the resected specimen
Note 1: Use this rule only when there are multiple polyps. Do not use for a single polyp (adenoma) or for a de novo (frank)
malignancy and a malignancy in a single polyp.
Note 2: Use this rule ONLY for adenocarcinoma in FAP.
Note 3: The disease process, treatment, and prognosis for FAP is not as favorable as a single polyp with adenocarcinoma.
Colon Solid Tumor Rules
September 2021 Update
36

Colon, Rectosigmoid, and Rectum Histology Rules
C180-C189, C199, C209
(Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140)
Jump to Equivalent Terms and Definitions
Jump to Multiple Primary Rules
Rule H13 Code adenocarcinoma in multiple adenomatous polyps 8221 when FAP is not mentioned AND
• There are at least 2 polyps with adenocarcinoma /2 or /3 AND
ο Less than or equal to 100 polyps are identified OR
ο The exact number of polyps is unknown/not documented
Note 1: Do not use this code for a malignancy in a single polyp (adenoma) or for a de novo (frank) malignancy.
Note 2: Use this rule ONLY for adenocarcinoma NOS in multiple polyps.
Rule H14 Code the histology of the invasive tumor when there are in situ /2 and invasive /3 tumors.
• One tumor is in situ and the other is invasive
• All tumors are a mixture of in situ and invasive histology
Rule H15 Code the histology when only one histology is present in all tumors.
Note 1: Use Table 1 to code histology. New codes, terms, and synonyms are included in Table 1 and coding errors may occur if
the table is not used.
Note 2: When the histology is not listed in Table 1, use the ICD-O and all updates.
Note 3: Submit a question to Ask a SEER Registrar
when the histology code is not found in Table 1, ICD-O or all updates.
Rule H16 Code the subtype/variant when the diagnosis is a NOS and a single subtype/variant of that NOS such as the following:
• Adenocarcinoma 8140 and a subtype/variant of adenocarcinoma
• Mixed adenoneuroendocrine carcinoma 8244 and a subtype/variant of mixed adenoneuroendocrine carcinoma
• Neuroendocrine carcinoma 8246 and a subtype/variant of neuroendocrine carcinoma
• Neuroendocrine tumor Grade 1 (G1) 8240 and a subtype/variant of neuroendocrine tumor Grade 1 (G1)
• Sarcoma 8800 and a subtype/variant of sarcoma
Note 1: All tumors may be mixed histologies (NOS and a subtype/variant of that NOS) OR one tumor may be a NOS histology
and the other tumor a subtype/variant of that NOS.
Note 2: See Table 1
in the Equivalent Terms and Definitions to find NOS and subtypes/variants.
Note 3: Check the Multiple Primary Rules to confirm that the tumors are a single primary.
Note 4: Only code subtypes/variant when pathology gives an exact diagnosis. Do not code the subtype/variant when modified by
terms such as differentiation, features of, etc., unless there is a specific code for the histology term with the modifier.
This is the end of instructions for Multiple Tumors Abstracted as a Single Primary.
Code the histology using the rule that fits the case.
Colon Solid Tumor Rules
September 2021 Update
37

{kind=link}