
The Business Case for Medical Respite Services
Donald S. Shepard
1
and Dan Shetler
2
1
Brandeis University, Waltham, MA
2
Columbus House, New Haven, CT
Corresponding author:
Donald S Shepard
Heller School MS 035
Waltham, MA 02454-9110
www.brandeis.edu/~shepard
Tel 781-736-3975
shepard@brandeis.edu
20 December 2016

2
TABLE OF CONTENTS
EXECUTIVE SUMMARY .................................................................................................................................. 3
OVERVIEW ................................................................................................................................................. 3
BACKGROUND ........................................................................................................................................... 3
RESULTS .................................................................................................................................................... 5
LIMITATIONS ............................................................................................................................................. 5
RECOMMENDATIONS ............................................................................................................................... 5
MAIN REPORT ............................................................................................................................................... 7
INTRODUCTION ......................................................................................................................................... 7
METHODS .................................................................................................................................................. 8
RESULTS FOR ST. FRANCIS HOSPITAL (HARTFORD, CT) .......................................................................... 10
RESULTS FOR HOLY CROSS HOSPITAL (FT. LAUDERDALE, FL) ................................................................. 13
DISCUSSION ............................................................................................................................................. 16
ACKNOWLEDGMENTS ............................................................................................................................. 18
APPENDIX 1: DETAILED METHODS .............................................................................................................. 19
APPENDIX 2: ADDITIONAL RESULTS - ST. FRANCIS HOSPITAL .................................................................... 21
APPENDIX 3: ADDITIONAL RESULTS FROM HOLY CROSS HOSPITAL ........................................................... 29
APPENDIX 4: ADDITIONAL RESULTS FROM COMPARISON ......................................................................... 35
REFERENCES ............................................................................................................................................ 36

3
EXECUTIVE SUMMARY
OVERVIEW
The objective of this study is to develop a business case for medical respite (MR). This business case
examines the potential costs and financial benefits of MR care to hospitals treating patients
experiencing homelessness, particularly those in Trinity Health. Although providing medical care to
people experiencing homelessness is part of a hospital’s social mission, individuals in this population are
difficult to identify and represent a substantial financial burden to the hospitals that treat them.
Using the capture-recapture method to estimate more accurately the number of episodes of patients
experiencing homelessness, the best estimate is actually 2.0 to 2.3 times the numbers that were
identified. Furthermore, we found that the full cost of care for this population exceeds the
reimbursement the hospital receives; thus, on average, the hospital loses money on each episode. If MR
can treat patients experiencing homelessness less expensively, MR can help reduce the hospital’s costs.
In addition, if the hospital is part of an accountable care organization (ACO) or similar shared savings
arrangement, it may gain additional revenues through shared savings.
Taking into consideration a standard MR model, we calculated that St. Francis Hospital (in a Medicaid
expansion state) could afford to contribute up to $4,635 and Holy Cross Hospital (in a non-expansion
state) could contribute up to $8,268 towards an episode of MR, and still break even. In a national study
for the Centers for Medicare and Medicaid Services, an average episode of MR lasted 45 days and cost
$136 per day or $6,120 in total.
1
Our financial analysis suggests that in a non-Medicaid expansion state,
a hospital will benefit financially from MR care even if it paid the full cost of MR care. In a Medicaid
expansion state if both the hospital and payers each paid 50% of the cost, both stakeholders would
benefit financially from MR. Therefore, we recommend that in these states, hospitals and payers
collaborate to fund MR programs, which will result in improved care for patients experiencing
homelessness, and financial savings and reduced risk for both parties.
BACKGROUND
Setting
Hospitals treat persons experiencing homelessness as part of their social responsibility. The project
conducted case studies in two hospitals to examine the situation in a state with Medicaid expansion, St.
Francis Hospital, (Hartford, CT), and one without expansion, Holy Cross Hospital (Ft. Lauderdale, FL). MR
care provides a safe place for people experiencing homelessness to continue to receive medical care
after a hospital visit without the high costs associated with prolonged hospital stays. MR services are
thought to not only improve health outcomes for persons experiencing homelessness, but also generate
savings for acute care hospitals and/or the health care system that makes it financially viable for them.
Payment models for MR are currently the subject of active discussion by hospitals, health centers, and
stakeholder associations.
2
If a hospital belonged to a Next Generation ACO, a shared risk payment model
under which healthcare providers can retain 80%-100% of generated savings, an MR program could
potentially not only reduce costs but also generate revenue to hospitals.
3

4
Approach
Although some people experiencing homelessness self-identify, many choose to “fly under the radar” or
hospital staff may not be asking the right questions to elicit a person’s true housing status. Without
knowing an accurate volume of patients who are experiencing homelessness, any financial analysis
would underestimate the full cost of caring for this population. To overcome this obstacle we employed
the capture-recapture methodology, which allows us to estimate the total size of a population based on
the size and overlap between two independent samples.
4
Having estimated the net losses incurred by caring for this population, we turned to estimating the
potential savings that MR could represent. There are two main areas where MR can potentially generate
savings. Experts on homelessness estimate that the average length of stay of patients experiencing
homelessness is about two days longer than is typical for housed patients. The first area of savings rests
on the estimate that, had an MR
facility been available, these two
extra days in the hospital could be
eliminated. The other area of savings
rests on interim findings from a
federally funded study. It found that
among MR participants experiencing
homelessness, the average the rate
of hospital admissions declined by
35% in the year following MR care as
compared to the year before, and
that average emergency room visits
dropped 45% in the same time
period.
1

5
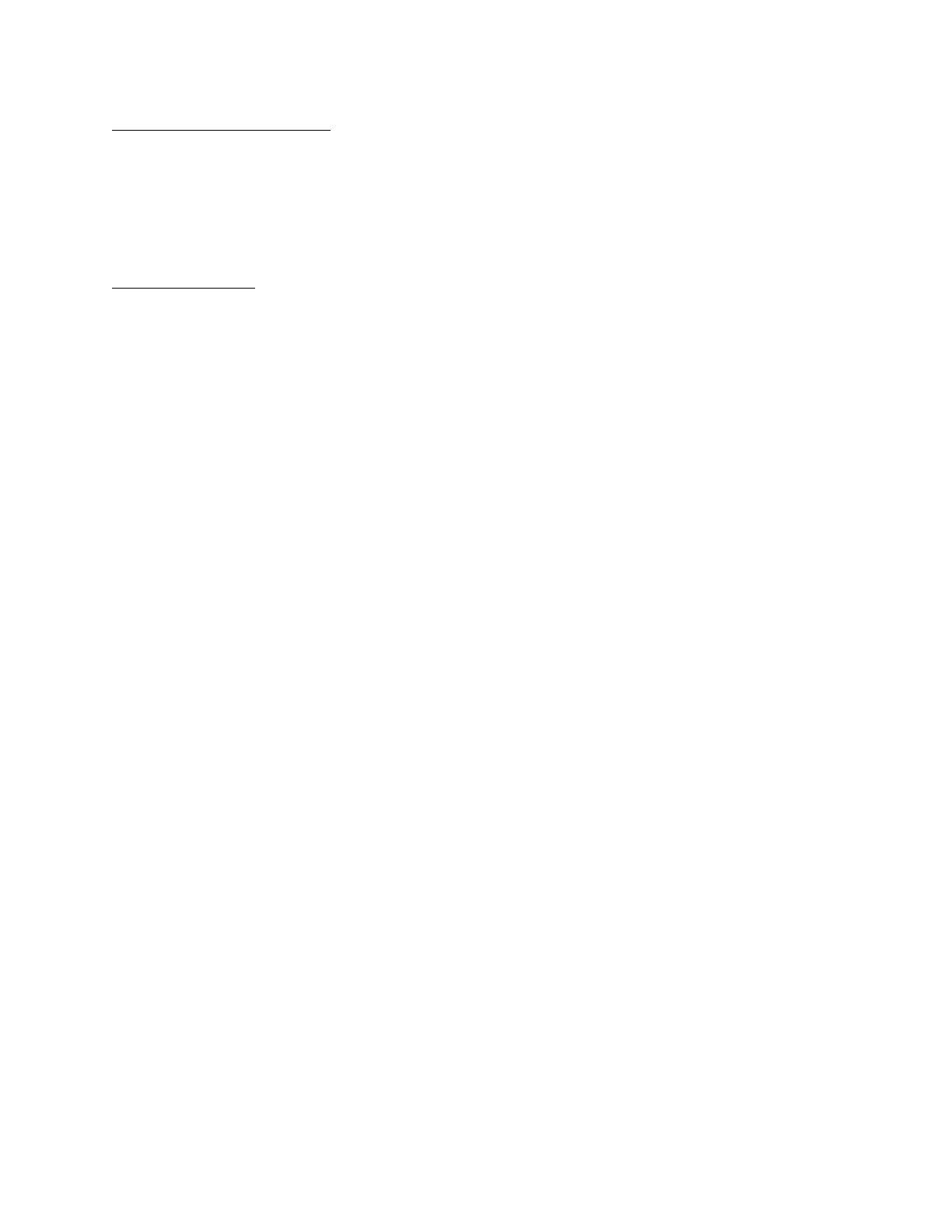
RESULTS
Using the capture-recapture method,
the projected numbers of annual
homeless episodes were 3,328 and
1,927 episodes, at St Francis and Holy
Cross respectively, or 2.3 and 2.0
times the identified numbers. While
hospitals receive reimbursement for
some of these patients experiencing
homelessness, both hospitals lost
money on their care, in the sense
that reimbursement was less than
the full cost (see Figure A). Given the
average reimbursement as a
percentage of complete cost, we
found that St. Francis is realizing an
annual net loss of $3.3 million and
Holy Cross, an annual net loss of $2.7
million by serving this population.
MR would reduce these losses,
thereby saving the hospitals money.
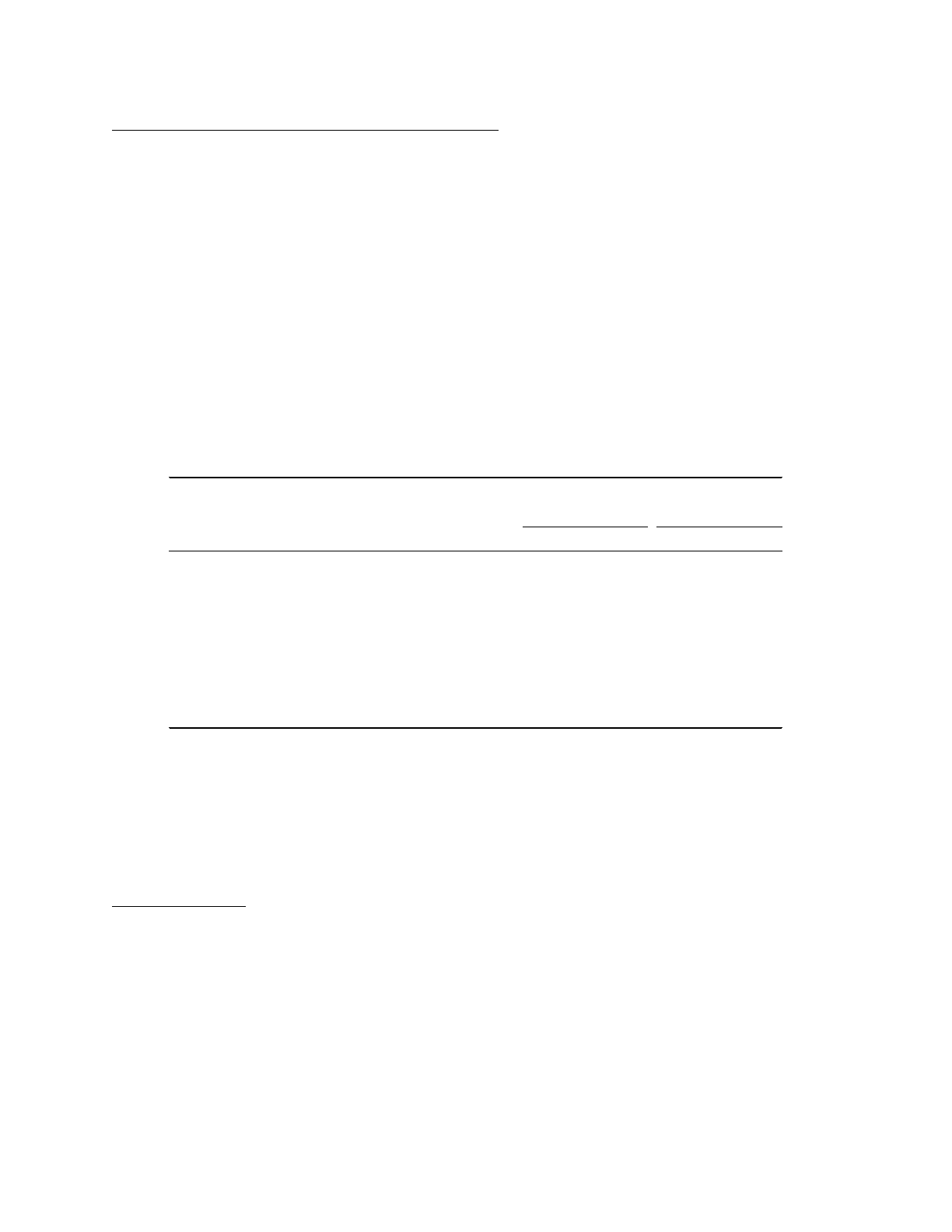
Taking into account a standardized
MR model, Figure B shows the estimated savings and their use per MR admission. Each hospital saves
money from three sources: a 2-day reduction in length of stay, fewer subsequent inpatient admissions
after discharge and fewer subsequent emergency room episodes after discharge.
LIMITATIONS
Three limitations should be acknowledged. First, part of this analysis is based on the assumption that
MR will eliminate two days from the average hospitalization. This can only be achieved through tight
coordination of care between the hospital and MR program, and should be monitored and refined as
the program is implemented. Second, this study analyzed only two hospitals in Trinity Health.
Extrapolation to other hospitals should take into account the particularities of those hospitals. Third, we
have projected the cost of an MR episode in an average-cost program. Costs of actual MR programs vary
by a factor of two.
RECOMMENDATIONS
Medicaid expansion states
In Medicaid expansion states, where Medicaid is already reimbursing much of the cost of care for this
population, both hospital and payer will realize savings if the cost of MR care is split between these two
parties (or subsidized by other funders). Therefore, it is recommended that Medicaid and hospitals
collaborate to fund MR programs jointly. This cooperation will financially benefit both parties.
Figure B. Estimated savings and their use per medical respite
admission
6
Non-Medicaid expansion states
On the other hand, the analysis suggests that in non-Medicaid expansion states, hospitals will realize
savings from funding MR programs even if the hospital were to fund the full cost of MR. This result is in
part due to the high cost of charity care in non-Medicaid expansion states. Therefore it is recommended
that in these states, it is in the hospital’s best interest to help initiate and fund MR programs, regardless
of other funding sources.
Risk-based contracts
In addition to savings realized directly by hospitals from MR, some risk-based payment models can share
the payers’ savings with the hospitals that help generate them. Next Generation ACOs, for example, will
pay providers 80% to 100% of generated savings as additional revenue.
3
Although only a small portion
of people experiencing homelessness are Medicare beneficiaries, the revenue generated from a
Medicare Next Generation ACO is likely relatively small. Some Medicaid contracts may have similar
arrangements, thereby generating greater additional revenue.

7
MAIN REPORT
INTRODUCTION
Homelessness increases use of inpatient and emergency department (ED) care. People experiencing
homelessness have high readmission rates: 30-day ED revisit rates are 5.7 times higher, and 30-day
inpatient readmission rates are 1.9 times higher than their housed counterparts.
5
They also stay in the
hospital longer than their housed counterparts. Patients in New York City experiencing homelessness
stayed 4.1 days (36%) longer and cost an average of $4,094 more than their housed counterparts,
adjusted for case mix, demographics and socio-economic characteristics.
6
A Toronto study using
administrative data found that admissions of patients experiencing homelessness on average cost
$2,559 (Canadian dollars, approximately the same in 2011 US dollars) more than their housed
counterparts after adjusting for individual characteristics and resource intensity weight.
7
Among all
inpatients experiencing delay in discharge days (hospitalizations prolonged due to non-medical or
external causes), homeless patients experienced 4 more delay days than their housed counterparts.
8
Patients experiencing homelessness also tend to use the ED for regular care in lieu of primary care,
contributing to both higher hospitalization costs and elevated mortality.
9, 10
A national study found
patients experiencing homelessness averaged 6.0 ED visits per year compared to 1.6 visits for housed
counterparts, and 24.6% encountered barriers to receiving needed medical care within the past year.
11
One driver of these trends is these patients’ lack of access to a safe, sanitary space to convalesce and
receive post-acute care.
12, 13
Medical respite (MR) programs have been developed to provide such a
space. They seek to break the cycle of hospital to homelessness, ease the suffering of this vulnerable
population and reduce medical system costs. In experience to date, a randomized trial in Chicago found
that MR paired with permanent supportive housing reduced hospital length of stay by 2.7 days, reduced
hospitalizations by 29%, and reduced emergency department visits by 24%.
14
A retrospective cohort
study in Boston, controlling for individual characteristics, found that MR lowered the odds of hospital
readmission by roughly 50%.
15
Interim findings from a national study found that MR reduced
subsequent inpatient admissions by 35% and subsequent ED visits by 45%.
1
Chicago patients discharged
to MR with subsequent supportive housing saved the health system $6,307 over patients discharged to
usual care.
16
While these studies show the potential of MR for improving outcomes and saving costs, they have
several limitations. The latest published study dates from 2012, before most provisions of The
Affordable Care Act took effect, so they do not reflect the current health care environment. Also, they
examine the health system as a whole. To become a sustainable service, MR would need a long-term
payment model. Such models are currently the subject of active discussion by hospitals, health centers,
and stakeholder associations.
2
Alternative payment models, particularly Next Generation Accountable
Care Organizations (ACOs) and similarly designed Medicaid contracts, can provide a mechanism for
hospitals to obtain additional revenue from MR. MR programs can be funded as part of the medical
services delivered by a Federally Qualified Health Center, reimbursed as fee-for-service, paid on a flat
rate by a managed care plan, supported by a grant, or funded by hospitals or payers (private insurers,
managed care organizations and government programs).
To inform these multi-party decisions, costs and savings need to be separated by payer. To address
these needs, we develop a business case for MR. We examine the potential costs and financial benefits

8
of MR to hospitals treating patients experiencing homelessness and the payers in their healthcare
markets. Using two Trinity Health hospitals as examples, we consider states both with and without
Medicaid expansion under the Affordable Care Act.
METHODS
Study hospitals
Trinity Health selected two hospitals in its network for site-level analysis: St. Francis Hospital (Hartford,
CT) and Holy Cross Hospital (Ft. Lauderdale, FL). St. Francis Hospital is a 617-bed, acute care hospital;
Holy Cross Hospital is a 557-bed, acute care hospital. With Connecticut being a Medicaid expansion state
and Florida not, the two hospitals represent a range of contexts for this study. Staff of Yale New Haven
Hospital, who have developed detailed procedures for identifying patients experiencing homelessness
and examining service utilization, provided additional methodological insights.
Number of care episodes of patients experiencing homelessness
Although some people experiencing homelessness self-identify, many are not recognized. Some patients
may choose to “fly under the radar” while others may not have been asked the appropriate questions to
elicit their true housing status. Without knowing the complete number of care episodes to patients
experiencing homelessness, any financial analysis would underestimate the full cost of caring for this
population. To overcome this obstacle, we employed the capture-recapture methodology, which allows
us to estimate the total size of a population based on the size and overlap between two independent
samples.
4
Both hospitals began to identify patients who were experiencing homelessness using information from
their medical record system during the year ending April 30, 2016. St. Francis first searched for the word
“homeless” in its Epic electronic medical record system and Holy Cross the “code 17”
i
in its Meditech
electronic medical record system.
The second independent sample relied on identifying patients experiencing homelessness via an
International Classification of Diseases (ICD) diagnosis code (V60 in ICD-9 or Z59 in ICD-10) which
represents homelessness. These codes are generally completed by the responsible provider on
discharge. Both St Francis and Holy Cross have been able to use this approach. Treating the two
approaches as independent, we implemented the capture-recapture technique with data from each
hospital by type of episode, and then summed across types of episode. This allowed us to estimate the
total number of episodes of people experiencing homelessness at each hospital (including those who
had not been identified as such).
Potential financial savings
To describe the current costs of treatment for patients experiencing homelessness, patients were
grouped by financial category, such as Medicaid or self-pay. The hospitals reported charges and, where
available, revenues and costs.
Having estimated the costs incurred by caring for this population, we turned to estimating the potential
savings that MR could represent. There are two main areas were MR can potentially generate savings.
i
Code 17 is used at Holy Cross Hospital to identify patients experiencing homelessness.

9
Based on expert opinion, consistent with data from St. Francis Hospital and Yale New Haven Hospital,
we estimated that patients experiencing homelessness were hospitalized for two days longer than
housed patients with comparable diagnoses (Michael Ferry and Janis Bozzo, unpublished data from Yale
New Haven Hospital, Aug. 2016). This is consistent with previous studies.
6-8
The first area of savings rests on the estimate that, had an MR facility been utilized, these two extra days
in the hospital could be eliminated. The average costs from the second to last day of these episodes
represent a good estimate of the daily costs associated with a patient who is ready to be discharged but
is being held in the hospital because a safe discharge destination has not been arranged. Doubling these
costs thus estimates the savings that would be realized by shortening an episode by two days. This
approach reduced the chance of spurious findings due to a partial stay or late billings, which could have
affected the actual charges and costs associated with the last two days.
The other area of savings rests on interim findings from a federally funded study from a standardized
program of MR. Preliminary results across five sites found that the average length of stay was 45 days.
The average rate of hospital admissions for MR participants dropped from 0.13 to 0.08 per person per
month from the year before to the year after MR, a 35% decline. Similarly, the average rate of
emergency room visits dropped from 0.33 to 0.18 per person per month from the year before to the
year after this period, a 45% decline.
1
Finally, we conducted sensitivity analyses to reflect the possible distribution of the costs of an MR
program between the hospital that typically treats patients experiencing homelessness and the funder.
See Appendix 1 for more details on the methodology.
We used data from Yale New Haven Hospital which allowed us to estimate the likely use of MR. Out of
1,496 inpatient admissions of persons identified as experiencing homelessness, during 2014-15, 8.0%
(204) entered MR. The remainder were not eligible (e.g., did not require daily medical care) or declined
to participate (e.g., could not agree to the program’s rules such as the inability to come and go from the
program at will, etc.). The above study of MR found an average length of stay of 45 days. We estimated
that in order to be efficient, but always have a bed available for an admission when needed, an MR
program could operate at an occupancy rate of 80%.
1
This means that over the year, one MR bed allows
6.49 admissions. Based on a daily cost of $136 per occupied bed, the annual cost of one bed would be
$39,700. If the hospital paid 50% of this cost, its annual share would be $19,850 per respite bed.

10
RESULTS FOR ST. FRANCIS HOSPITAL (HARTFORD, CT)
Number of care episodes of patients experiencing homelessness
Figure 1 shows the application of the search procedures and the capture-recapture technique to St.
Francis Hospital. The results indicate that only about one in three likely homeless patients is currently
being identified as experiencing homelessness. These capture-recapture calculations suggest that St.
Francis hospital provided 3,328 care episodes to patients experiencing homelessness (665
hospitalizations and 2,663 outpatient visits). For details see Appendix 2, Table A4.
Figure 1: Numbers of episodes at St. Francis Hospital of patients experiencing homelessness, 2015-16.
Legend: Episodes of encounters of patients experiencing homelessness were identified through
addresses (n=1035), diagnoses (n=562), both sources (n=140) or either source (n=1457), and projected
using the capture-recapture method (n=3,328).

11
Projected financial impacts of shorter hospitalization
The length of stay of patients experiencing homelessness in St. Francis Hospital of 5.75 days was about
two days longer than the hospital’s typical length of stay. We estimated the savings from a two-day
reduction in the inpatient hospital stay for relevant admissions. We excluded patients with a length of
stay of one or two days, as a two-day reduction would have made their length of stay negative or zero.
This exclusion removed 30 (3 with one day and 27 with two days) or 6.6% of the 455 identified
hospitalizations of patients experiencing homelessness. Table 1 shows the results. For further details,
see Appendix Table A4. The net revenue averaged $8,894. While this revenue covered the hospital’s
direct cost, it did not cover the complete cost.
ii
The last two days of care had average complete costs
(including indirect costs) of $1,933. The hospital lost $3,175 per hospitalization of three or more days.
Financial Class
Eligible
inpatient
stays
Avg.
LOS
Net
Revenue
Charges
Complete
cost*
Loss on
full stay
On
charges
On
complete
cost
Medicaid 329 7.0
$8,841 $26,211
$11,795 $2,953 $4,370
$1,967
Medicare
77 9.3 $9,244
$31,421 $14,139 $4,896
$3,504 $1,577
All Payers 425
7.4 $8,894 $26,820
$12,069 $3,175 $4,296
$1,933
Table 1. Amounts per inpatient admission, St. Francis Hospital
*Complete cost (including indirect costs) was estimated from the finding that inpatient cost averaged
45.0% of inpatient charges.
Actual hospitalizations
Savings from 2-day
reductIon
Notes: hospitalizations of fewer than 3 days were excluded. Avg. denotes average; LOS denotes length
of stay.
Almost all inpatient care is paid based on the discharge diagnosis for the episode, so the payment would
not be affected by a reduction in length of stay. If the hospital could save the costs associated with the
last two days, the average loss per patient would drop to $1,242 (i.e., $3,175 minus $1,933). Altogether,
savings from eliminating the last two days, counting direct and indirect costs, lowers the loss per
hospitalization of a patient experiencing homelessness by 61%. See Appendix 2, Table A6 for details.
ii
Direct costs relate to services directly received by patients, such as general ward care, prescriptions and
laboratory procedures. Indirect costs relate to supportive services, such as administration or insurance. Complete
costs were estimated from the finding that inpatient costs average 45% of inpatient charges at St. Francis Hospital.
12
Potential downstream impacts on health systems’ costs
Along with the savings associated with reducing the hospital length of stay, MR programs have the
potential to generate savings by reducing the number of hospitalizations in the year following an MR
admission.
15
Table 2 merges the savings from both the length of stay reduction and reduced subsequent
hospitalizations to assess the one-year savings to the two major health system stakeholders: the
hospital treating the patient and the primary payer (i.e., Medicaid) for the patient’s care. Under this
projection, the hospital will experience fewer inpatient and outpatient episodes in the subsequent year.
As the hospital would have incurred a loss on each of these episodes, the reduction in such episodes
represents a reduction in its loss—a relative savings. The hospital also gains from a shorter hospital stay.
This base case financial analysis assumes that the MR stay is funded half by the hospital and half by the
payer. In the previously mentioned respite study, the median cost per day was $136 with a wide range
of $60 to $388.
1
Using the median value, a 45 day admission to MR would cost $6,120 for an MR stay
that is split between the hospital and the payer. In this base case, the hospital saves $1,575 per respite
episode, while the payer saves $1,254 per respite stay. See Appendix 2, Table A7 for details.
Table 2. Projected financial impact of one medical respite (MR) episode, St. Fancis Hospital
Annual
Source of impact
Reduction Hospital Payer Hospital Payer
Fewer subsequent inpatient episodes 0.60 $3,322 $6,215
$1,993 $3,729
Fewer subsequent emergency episodes 1.80 $394
$325 $709 $585
2-day reduction in impatient stay $1,933 $0
-$3,060
-$3,060
Total $1,575 $1,254
Loss per MR
episode
Annual savings
from MR episode
Medical respite stay (50% each)
If St. Francis Hospital or a partner organization wished to set up an MR program to meet the hospital’s
needs, we estimate that it would have 117 MR admissions annually (1,457 identified homeless episodes
x 8.0%) and need 18 MR beds (117/6.49 admissions per bed). The annual cost of this respite program to
the hospital and payers would each be $357,000 (i.e., 18x$19,850, as noted above). After paying these
contributions, however, the hospital and payers would still realize a yearly net savings of $184,000 and
$147,000, respectively.
Sensitivity analyses
Our most likely assumption is that hospital and payer each fund 50% of the costs of MR. Then the
hospital saves $1,575 while payers gain $1,254 per MR admission. In the examination of alternative
allocation of costs of MR between the hospital and payers, we found that if the hospital’s share is
between 30% to 75% of the costs (so the payer’s share is 25% to 70%), then both parties realize financial
savings from MR. See Appendix 2, Figure A3 for details.

13
RESULTS FOR HOLY CROSS HOSPITAL (FT. LAUDERDALE, FL)
Number of care episodes of patients experiencing homelessness
Figure 2 shows the application of search procedures and the capture-recapture technique to Holy Cross
Hospital. The results indicate that only about half of the episodes by likely patients experiencing
homelessness are currently being identified. The capture-recapture calculations suggest that Holy Cross
Hospital provided 1,927 care episodes to patients experiencing homelessness (232 inpatient, 1,381
emergency and 314 observation visits). See Appendix 3, Table A10 for details.
Figure 2: Numbers of episodes at Holy Cross Hospital of patients experiencing homelessness, 2015-16
Legend: Episodes of encounters of patients experiencing homelessness were identified through
Admission “Code 17"
iii
(n=631), diagnoses (n=200), both sources (n=120) or either source (n=711), and
projected using the capture-recapture method (n=1,927).
Projected financial impacts of shorter hospitalization
We built on the assumption that a well-coordinated MR program would, on average, be able to
eliminate two medically unnecessary days of the hospital length of stay. Beginning with inpatient
episodes based on admissions criteria, we excluded 25 episodes with a length of stay of one or two days.
This left 117 of the original 142 episodes.
Almost all inpatient care is paid based on the discharge diagnosis for the episode, so the payment would
not be affected by a reduction in length of stay. Table 3 shows calculations of the savings associated
with eliminating two medically unnecessary days. These data show that the projected savings from a
two-day reduction in length of stay averaged $2,934, slightly smaller than the corresponding amount at
St Francis Hospital ($3,175). See Appendix 3, Table A11 for details.
iii
Code 17 is used at Holy Cross Hospital to identify patients experiencing homelessness

14
Table 3. Projected impact of a 2-day reduction in length of stay on a hospitalization of 3 or more days,
Financial
Class
Eligible
inpatient
stays
Avg.
LOS
Net
Revenue
Charges
Complete
cost
Loss on
full stay
On
charges
On
complete
costs
Medicaid
25 11.6 $8,452 $87,134 $28,014
$19,562
$8,951 $3,489
Medicare 38 8.7 $13,765
$79,564
$18,904 $5,139 $9,094 $2,885
All Payers 117 11.9 $9,568 $67,849 $18,368 $8,800 $8,646 $2,934
Savings from 2-day
reduction
Actual hospitalizations
Holy Cross Hospital
Notes: Hospitalizations of fewer than 3 days were excluded. Avg. denotes average; LOS denotes length
of stay.
Potential downstream impacts on health systems’ costs
As noted earlier, potential savings may be realized through shorter hospital stays and fewer hospital
encounters following an MR stay. Table 4 merges the savings realized through reducing an average of
two medically unnecessary days of hospitalization with the savings from reduced inpatient and ED visits
in the year after MR. This base case financial analysis assumes that the MR stay is funded half by the
hospital and half by the payer. In the previously mentioned respite study, the median cost per day was
$136 with a broad range of $60 to $388.
1
Using the median value, an admission to MR would cost
$6,120. Thus, the cost of 45 days at $138 per day or $6,120 for the MR stay is split between the hospital
and the payer. In this base case, the hospital saves $5,208 per respite episode, while payers save $1,885
per respite episode. See Appendix 3, Table A12 for details.
Table 4. Projected financial impact of one medical respite (MR) episode, Holy Cross Hospital
Annual
Source of impact Reduction Hospital Payer
Hospital Payer
Fewer subsequent inpatient episodes
0.60 $7,421 $7,928 $4,453 $4,757
Fewer subsequent emergency episodes
1.80 $490 $104 $881 $188
2-day reduction in inpatient stay $2,934 $0
-$3,060
-$3,060
Total $5,208 $1,885
Loss per MR
episode
Annual savings
from MR episode
Medical respite stay (50% each)
If Holy Cross Hospital or a partner wished to set up or expand an MR program to meet the hospital’s
needs, we estimate that it would have 57 admissions annually (711 identified homeless episodes x 8.0%)
and need 9 MR beds (57/6.49 admissions per bed). The annual cost of this respite program to the
hospital and payers would each be $179,000 (i.e., 9x$19,850, again as noted above). After paying these
contributions, however, the hospital and payers would still realize yearly net savings of $297,000 and
$107,000, respectively.
Sensitivity analyses
Our sensitivity analysis (see Appendix 3, Figure A5 for details) shows the effect on savings for both payer
and hospital as the hospital pays for a larger and larger share of the cost of MR. Ironically, as the

15
hospital in a non-Medicaid expansion state loses more money on each hospitalized episode of care for a
person experiencing homelessness, it could afford to pay more towards an MR stay and still benefit
financially. The threshold analysis shows that the payer saves, provided the hospital pays at least 19% of
the cost of MR. As the hospital pays a higher share of the costs of MR, its savings fall but still remain
positive (i.e., the hospital would realize savings even it paid for the full cost of the MR care episode).
RESULTS ON COMPARISON BETWEEN HOSPITALS
As a way of seeking to generalize beyond the two hospitals, we show results of the hospitals together.
Figure 3 shows the full cost of an average episode of inpatient care at each of the hospitals. It shows
that the episode costs more in Holy Cross Hospital. Additionally, being located in a state without
Medicaid expansion, the net loss of the hospital in Florida is higher in both dollar and percentage terms
than its Connecticut counterpart.

16
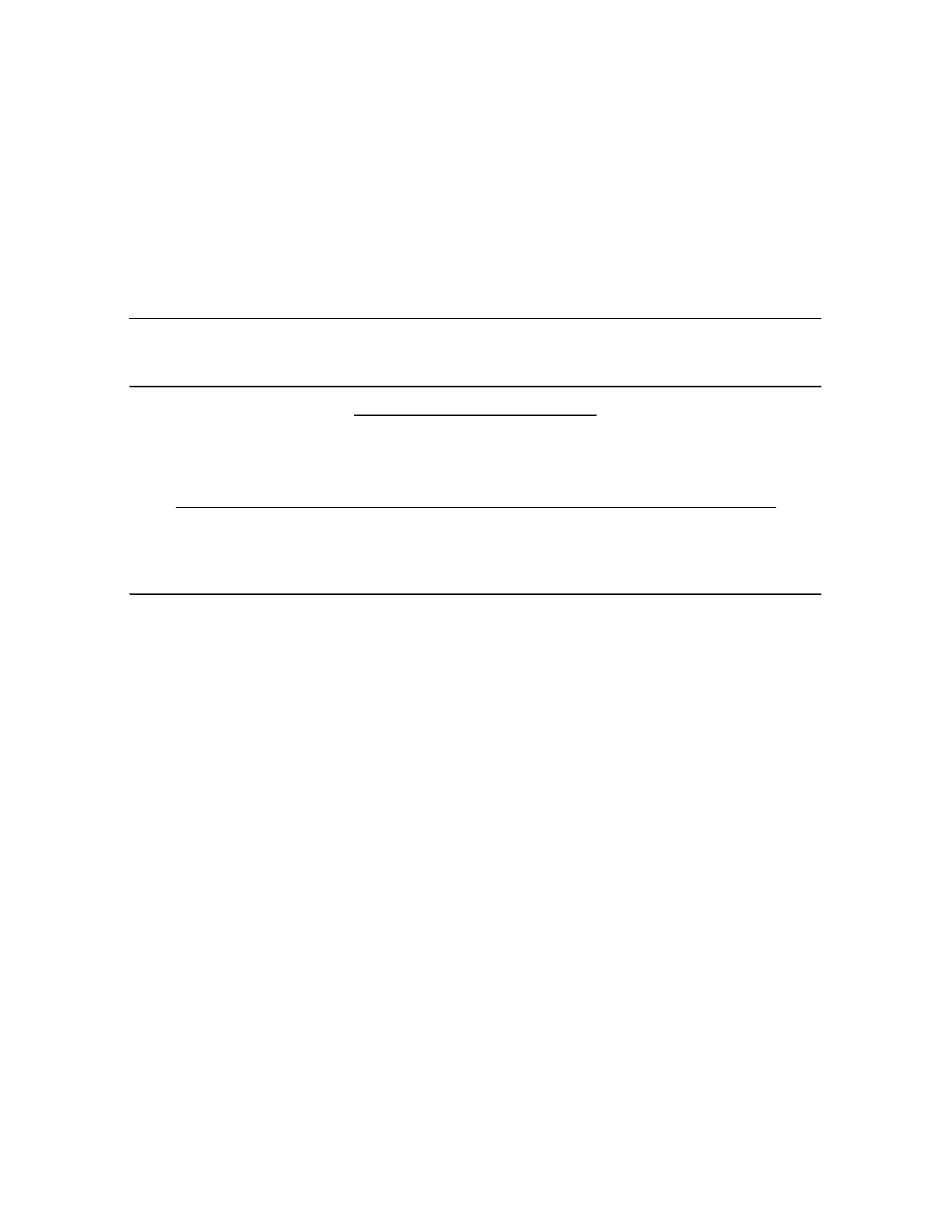
Figure 4 shows the estimated savings and their use per MR admission. Each hospital saves money from
three sources: fewer subsequent emergency room episodes after discharge, a 2-day reduction in length
of stay, and fewer subsequent inpatient admissions after discharge.
Figure 4. Estimated savings and their use per medical respite admission
DISCUSSION
Both of these hospitals serve their social missions by treating a substantial number of patients
experiencing homelessness. The care of these patients must be subsidized from other sources. The
specific number of patients experiencing homelessness served increases the more thoroughly the
hospital records are searched. At St. Francis Hospital, for example, the search under the word
“homeless” in the address field found 99 hospitalizations. When other relevant addresses (those of
shelters and the hospital) were added, the number of homeless hospitalizations increased to 142. When
homeless discharge diagnoses are added, the number rose to 455. Finally, using the capture-recapture

17
technique to adjust for patients experiencing homelessness who were not identified, the projected
number of hospitalizations rose to 665. The technique also raised the estimated number of outpatients
treated by the hospital. The projected 3,328 care episodes of patients experiencing homelessness at St.
Francis represents 5 episodes for each of the hospital’s 617 beds.
Even though almost all of the patients experiencing homelessness at St. Francis had an expected
payment source, the hospital lost money on their care as the reimbursement was low in relation to the
cost of their care. Overall, revenues average 58.3% of costs overall and 56.1% of costs for Medicaid
clients. For outpatients, reimbursement is even lower, being 45.2% of costs overall and just 40.6% for
Medicaid enrollees.
Results from the standardized model show several types of savings throughout the health care system.
An MR program with excellent coordination between the hospital and the MR program would plausibly
achieve a 2-day reduction in length of stay. Staff at Yale New Haven Hospital and its associated MR
program at Columbus House have not yet seen a reduction in inpatient length of stay of patients
experiencing homelessness compared to the period before the opening of MR (Ferry M, personal
communication, July 5, 2016). However, Columbus House has not previously had medical personnel on
its staff, but sees the potential for future reductions. On this assumption, MR could save an estimated
$1,933 on index admissions of patients experiencing homelessness at St. Francis. If the acute care
hospital did not have to pay for the MR program, the savings would substantially reduce the loss that
the hospital currently incurs.
Figure 4 presents the cost per case for both hospitals. The projected downstream impacts of MR on
subsequent inpatient and outpatient episodes involve considerable uncertainty. Here, we have taken
the direct before and after comparisons and applied them for a one-year period. Other factors could
make the true value higher or lower than this estimate. The factor leading to true savings being even
higher is the expectation that an MR program could have benefits longer than one year. Besides
addressing the current illness, a structured MR program seeks to connect clients to a medical home for
primary care (shifting long-term utilization habits from inappropriate emergency room visits to
preventative primary care visits), engage clients in smoking cessation, strengthen their self-confidence
and care management skills, and try to get them placed in permanent supportive housing. Successes
along these dimensions would likely persist for many years. On the other hand, our before and after
comparisons may be overstated due to regression to the mean, as clients generally entered MR at a
point of high utilization. For the present analysis, we have assumed that these two concerns would
offset one another.
This business case found that regardless of state’s Medicaid expansion, both payers and hospitals would
benefit financially if the costs of an MR program were shared roughly equally between these
stakeholders.
In addition to savings realized directly by hospitals from MR, some risk-based payment models can share
the payers’ savings with the hospitals that help generate them. Next Generation ACOs, for example, will
pay providers 80% to 100% of generated savings as additional revenue.
3
Although only a small portion
of people experiencing homelessness are Medicare beneficiaries, the revenue generated from a
Medicare Next Generation ACO is likely relatively small. Some Medicaid contracts may have similar
arrangements, thereby generating greater additional revenue. The savings and revenue are in addition

18
to the contribution of MR to the health and social wellbeing of people experiencing homelessness and
the community service goals of hospitals and payers.
ACKNOWLEDGMENTS
The authors thank the site coordinators and their colleagues at each of the study hospitals and at Yale
Haven Hospital. At St. Francis Hospital, they thank Rob Beeman, Jeffrey Joyce, Marcus McKinney (site
coordinator), and Khadija Poitras-Rhea, Adam Silverman. Suzanne Sullivan, and Lawrence Young. From
nearby Chrysalis Center, they thank Sharon Castelli. At Holy Cross Hospital, they thank Marlene Berger,
Amy B. Corderman (site coordinator), Kim Saiswick (site coordinator), Shailesh Jobanputra, and Julia E.
Greenwood. At Yale New Haven Hospital, they thank Janis Bozzo, Paula Crombie, and Michael Ferry.
They gratefully acknowledge Sabrina Edgington and John Lozier of the National Health Care for the
Homeless Council, Carrie A. Harnish and Antonio G. Beltran of Trinity HealthCare, and Tom Andrews of
Mercy Care (Atlanta, GA). At Brandeis University they thank Clare Hurley.
Financial support. This study was supported by Trinity Health through the National Health Care for the
Homeless Council.

19
APPENDIX 1: DETAILED METHODS
Study hospitals
As noted in the main text, Trinity HealthCare selected two hospitals in its network for site-level analysis:
St. Francis Hospital (Hartford, CT) and Holy Cross Hospital (Ft. Lauderdale, FL). St. Francis Hospital,
located at 114 Woodland St., Hartford, CT 06105, is a 617-bed acute care Catholic hospital (see Figure
A1). Holy Cross Hospital, located at 4725 N. Federal Highway, Ft. Lauderdale, FL 33308, is a 557-bed
acute care Catholic hospital (see Figure A2). With Connecticut being a Medicaid expansion state and
Florida not, the two hospitals represent a range of contexts for this study. Staff of Yale New Haven
Hospital, who have developed detailed procedures for identifying patients experiencing homelessness
and examining service utilization, provided additional methodological insights.
Figure A1. St. Francis Hospital
Figure A2. Holy Cross Hospital
Number of care episodes of patients experiencing homelessness
We first estimated the number of patients experiencing homelessness treated in the latest one year
period with data for both hospitals: the year ending April 30, 2016. To do this we employed the capture-
recapture technique, which allows us to estimate the total size of a population based on the size and
overlap between two independent samples.
4
Both hospitals began to identify these independent
samples by using information from their medical record system to identify patients experiencing
homelessness. St. Francis first searched for the word “homeless” in its Epic electronic medical record
system; and Holy Cross, the code 17
iv
in its Meditech electronic medical record system. St. Francis
subsequently expanded the registration search by checking for patients whose address on record
iv
Code 17 is used at Holy Cross Hospital to identify patients experiencing homelessness.

20
corresponded to the address of a homeless shelter in the greater Hartford area, or the hospital’s
address. Holy Cross’s staff were unable to search by address.
The second apparently independent sample relied on identifying patients experiencing homelessness via
the diagnosis code (V60 in ICD-9 or Z59 in ICD-10). These codes are generally completed by the
responsible provider on discharge. Both St Francis and Holy Cross have been able to use this approach.
Within each type of episode (inpatient and ambulatory), we considered the two approaches as
independent as the information came from different medical professionals with separate interaction
with the patient at different points during the episode care. Thus, we implemented the capture-
recapture technique with data from each hospital by type of episode, and then summed across types of
episode. This allowed us to estimate the total number of episodes of people experiencing homelessness
at each hospital (including those that had not been identified as such).
Potential financial savings
To describe the current costs of treatment for patients experiencing homelessness, patients were
categorized by financial category, such as Medicaid or self-pay. The hospitals reported charges and,
where available, revenues and costs.
As noted in the main text, to estimate the potential savings on inpatient admissions, we calculated the
resource use associated with “extra days” attributed to homelessness that might be eliminated by an
MR program. Based on expert opinion, consistent with data from Yale New Haven Hospital, we
estimated that patients experiencing homelessness were hospitalized for two days longer than housed
patients with comparable diagnoses (Michael Ferry, Janis Bozzo, unpublished data from Yale New Haven
Hospital, Aug. 2016). The associated financial implications were measured as the associated charges and
direct costs (reported directly) and as estimated total costs (derived through the ratio of inpatient costs
to charges). We examined overall costs and utilization with the concept of bed-day equivalents, where
one hospital outpatient visit is counted as 0.32 bed-day equivalents.
17
To project the financial impact of changes in utilization from MR, we estimated the average unit cost per
inpatient and outpatient episode. We used data from diagnostic categories that were treated entirely in
a single setting (either inpatient or outpatient), excluding categories that were managed in both
settings. We merged these unit costs with utilization data to estimate the one-year projected savings in
health systems’ costs following an MR episode. Finally, we conducted sensitivity analyses to reflect the
possible distribution of the costs of MR between the hospital that typically treats patients experiencing
homelessness and the payer.

21
APPENDIX 2: ADDITIONAL RESULTS - ST. FRANCIS HOSPITAL
Numbers and characteristics of care episodes
Table A1 shows the breakdown of patients experiencing homelessness at St. Francis based on the initial
registration information. It uses the bed-day equivalent as a unit of care combining both inpatient and
outpatient services, with weights derived from a review of hospital costs.
17
Almost all of the care (83.1%
of the bed-day equivalents) was for Medicaid beneficiaries. Although the hospital was paid for treating
Medicaid patients, Medicaid reimbursement covered only 57% of the costs. For Medicaid patients
experiencing homelessness the average cost was $1,871 per bed-day equivalent.
Payer (Financial Class)
Private (Blue
Cross,
Commercial,
Managed
Care)
Medicaid
Medicare
Managed
Care
Other
Welfare
Self Pay Total
Stays
Inpatient stays 3 83 11 2
0 99
Out-patient stays 4 441 38 3 15 501
Inpatient bed days 18 473 73 5 0 569
Bed-day equivs* 19.28 614.12 85.16 5.96 4.80 729.32
% distribution
Inpatient stays 3.0% 83.8% 11.1% 2.0% 0.0% 100.0%
Out-patient stays 0.8%
88.0% 7.6% 0.6% 3.0% 100.0%
Inpatient bed days 3.2% 83.1% 12.8% 0.9%
0.0% 100.0%
Financial aggregate amounts
Aggregate charges $69,384 $3,426,849 $365,670 $34,602 $72,925
$3,969,430
Aggregate costs $27,478 $1,148,977
$147,669 $9,979 $10,972 $1,345,075
Aggregate net revenue $30,095 $651,590 $97,737 $4,854 $333 $784,609
Aggregate net margin
$2,618 -$497,387 -$49,932 -$5,125 -$10,639 -$560,465
Avg. LOS 6.00 5.70 6.64 2.50
0.00 5.75
Cost as % of charges 39.6% 33.5% 40.4% 28.8% 15.0% 33.9%
Net revenue as % of charges 43.4% 19.0% 26.7% 14.0% 0.5% 19.8%
Net revenue as % of costs 109.5% 56.7% 66.2% 48.6% 3.0% 58.3%
Average charge per day equiv
$3,599 $5,580 $4,294
$5,806
$15,193 $5,443
Average cost per day equiv $1,425 $1,871 $1,734 $1,674 $2,286 $1,844
Average revenue per day equi
$1,561 $1,061 $1,148 $814 $69 $1,076
Payer % of bed-day equiv. 2.6% 84.2% 11.7% 0.8% 3.0% 100.0%
Payer % of charges 1.7% 86.3% 9.2% 0.9% 1.8% 100.0%
Payer % of costs 2.0% 85.4% 11.0% 0.7% 0.8% 100.0%
Payer % of revs 3.8% 83.0% 12.5% 0.6% 0.0% 100.0%
Payer % of net losses -0.5%
88.7% 8.9% 0.9% 1.9% 100.0%
*Each outpatient visit weighted as 0.32 bed day equivalents, based on Shepard et al (2000), Hospital
Table A1. Stay episodes in St Francis Care, Hartford, CT by financial group with "homeless" in
address field (May 1, 2015-April 30, 2016)
Notes: Equiv and Equ denotes equivalent; Avg. denotes average; LOS denotes length of stay; revs
denotes revenues.

22
Table A2 lists the leading diagnoses at St. Francis Hospital. The ranking is based on the number of
episodes, summing inpatients and outpatients. The ranking depends in part in the way that diagnoses
are grouped. Thus all of the top five categories contain the word “unspecified,” indicating the breadth of
these residual categories. It is noteworthy that all of the top five categories relate to behavioral health,
confirming the prominence of these conditions among patients experiencing homelessness.
Rank Diagnosis code & name
In-
patients
Days
Out-
patients
Epi-
sodes
Charges Total Cost
Net
Revenue
1
F10.129 Alcohol abuse
with intoxication,
0 0 21 21 80,255 15,368 6,558
2
F10.10 Alcohol abuse,
uncomplicated
0 0 15 15 57,619 11,082 4,218
3
303.00 AC Alcohol intox-
unspec
0 0 12 12 51,882 11,168 4,061
4
305.00 Alcohol abuse-
unspec
0 0 12 12 53,020 11,144 4,314
5
F20.9 Schizophrenia,
unspecified
2 17 10 12 83,985 35,674 19,270
All 99 569 501 600 3,969,430 1,345,075 784,609
Table A2. Leading diagnoses at St. Francis Hospital, ranked by number of episodes`with
address as "homeless"
Notes: unspec denotes unspecified

23
Table A3 shows the breakdown of care by setting at St. Francis Hospital. As the table was derived from
the combined breakdown by diagnosis and settings, it shows three settings: inpatient, mixed, and
outpatient. Mixed diagnoses were those that applied to both inpatient and outpatient episodes of
patients experiencing homelessness. This breakdown shows that costs are a higher percentage of
charges for inpatient care than for outpatient care. It also shows that inpatient care is better
reimbursed: revenue as a percentage of costs is higher for inpatient care compared to outpatient care.
The cost per bed-day equivalent is relatively similar between outpatient and inpatient services, $2,246
vs. $1,742, respectively.
17
Table A3. Breakdown of episodes by setting with patient's address as "homeless", St. Francis Hospital
Set-
ting
In-
pts
Days
Out-
pts
Charges Total Cost
Net
Revenue
Avg
LOS
Bed-
day*
equivs
Cost
%
chrgs
Net
rev %
chrgs
Rev %
costs
Cost/
bed-
day eq
All financial categories
Outpt 0 0 444 $1,623,101 $319,171 $144,281 0.0 142 19.7% 8.9% 45.2% $2,246
Mixed 40 246 57 $1,095,843 $463,230 $273,628 6.2 264 42.3% 25.0% 59.1% $1,753
Inpt 59 323 0 $1,250,487 $562,674 $366,700 5.5 323 45.0% 29.3% 65.2% $1,742
Total 99 569 501 $3,969,430 $1,345,075 $784,609 5.7 729 33.9% 19.8% 58.3% $1,844
Medicaid patients
Outpt 0 0 387 $1,401,568 $284,445 $115,594 0.0 124 20.3% 8.2% 40.6% $2,297
Mixed 37 227 54 $1,017,537 $428,487 $257,791 6.1 244 42.1% 25.3% 60.2% $1,754
Inpt 46 246 0 $1,007,744 $436,045 $278,205 5.3 246 43.3% 27.6% 63.8% $1,773
Total 83 473 441 $3,426,849 $1,148,977 $651,590 5.7 614 33.5% 19.0% 56.7% $1,871
*Each outpatient visit as weighted as 0.32 bed day equivalents, based on Shepard et al (2000), Hospital
Costs.
Notes: Inpt denotes inpatient; Outpts denotes outpatients; Avg denotes average; LOS denotes length of
stay; chrgs denotes charges; rev denotes revenues; eq denotes equivalent
If bed-day equivalent were a perfect measure of hospital resource use, then the cost per bed-day
equivalent would be identical between inpatient and outpatient settings. The similarity in unit costs per
bed-day equivalent between inpatient and outpatient settings indicates that the bed-day equivalent was
a reasonably good indicator of a unit of service in this study (Table A3). Cost patterns in mixed settings
were, as expected, intermediate between outpatient and inpatient settings.

24
Potential downstream impacts on health systems costs
Table A4 shows the capture-recapture analysis by setting.
Homeless
diagnosis*
No Yes Total
Number of
identified
encounters
Number of
projected
encounters
Expansion
factor from
identified
encounters
Expansion
factor
from
address
Inpatients
No Unknown 57 57
Yes 313 85 398
Total 313 142 455 455 665 1.5 4.7
Outpatients
No Unknown 838 838
Yes 109 55 164
Total 109 893 1002 1,002 2,663 2.7 3.0
Combined
No Unknown 895 895
Yes 422 140 562
Total 422 1035 1457 1,457 3,328 2.3 3.2
* Notes: ICD9-V60 or ICD10-Z59.
Address sources
Number %
Word "homeless" 629 19%
Word "shelter" or a shelter address 406 12%
Subtotal: all address fields 1,035 31%
Diagnosis code, excluding previously identified
422 13%
Subtotal: all identified patients 1,457 44%
Projected total 3,328 100%
Table A4. Application of 'capture-recapture' method to estimating number of care episodes to
patients experiencing homelessness, St. Francis*
Address "Homeless" or
Shelter
Application of capture-recapture

25
The upper panel in Table A5 shows the average cost of inpatient and outpatient episodes at St. Francis
Hospital based on episodes identified by searching for “homeless” in the address field. Because the
hospital’s net revenue is below its cost, the hospital incurs a loss on each episode of care provided to a
person experiencing homelessness. This loss occurs even if that patient is covered by Medicaid and the
hospital receives the Medicaid reimbursement. For all payers, reimbursement for an average inpatient
and outpatient episode covers only 65% and 45% of the costs, respectively. For Medicaid clients, these
percentages are slightly lower. The lower panel in Table A5 shows the aggregate amounts based on
projected episodes. Table A6 shows the details of the impact of a 2-day reduction in length of stay and
Table A7 the details of the impact of an MR episode.
Financial
class
Charges Cost Net revenue
% of
cost
Savings or loss (N)
All $21,195 $9,537 $6,215 65% -$3,322 59
Medicaid $21,907 $9,479 $6,048 64% -$3,431 46
All $3,656 $719 $325 45% -$394 444
Medicaid $3,622 $735 $299 41% -$436 387
Inpatient $14,094,467 $6,342,007 $4,133,147 65% -$2,208,860 663
Outpatient
$9,734,950 $1,914,304 $865,361 45% -$1,048,944 2,663
Total $23,829,417 $8,256,311 $4,998,508 61% -$3,257,803 3,328
Average per inpatient admission
Average per outpatient episode
Table A5. Average and aggregate amounts by type of episode, St. Francis Hospital
Aggregate amounts based on projected episodes

26
Table A6. Projected impact of a 2-day reduction in length of stay (LOS) of eligible hospitaliziations, St. Francis Hospital
Financial Class
Elig-
ible
inpt.
stays
Avg.
LOS
Net
Reve-
nue
Charges
Direct
Cost
Full com-
plete
cost*
Last 2
days:
charges
Last 2
days:
direct
cost
Last 2
days:
complete
cost
Savings
(loss)
complete
stay
Savings in
direct
costs (2
last days)
Savings in
complete
costs (2
last days)
Medicaid
All Medicaid 329 7.0 $8,841 $26,211 $5,500 $11,795 $4,370 $1,048
$1,967 -$2,953 -$1,906 -$987
Medicare
Medicare 62 8.8 $7,849 $24,779 $5,818 $11,150 $3,328 $866 $1,498 -$3,301 -$2,435
-$1,803
Medicare
Managed Care
15 11.1
$15,006 $58,876 $12,347 $26,494 $4,231 $1,095 $1,904 -$11,488 -$10,393 -$9,584
Other
Blue Cross 1 8.0 $6,888 $20,635 $5,400 $9,286 $2,693 $805 $1,212 -$2,398 -$1,593 -$1,186
Managed Care 6 6.8 $9,129 $18,966 $4,830 $8,534 $3,088 $919
$1,390 $594 $1,514 $1,984
Other Welfare 11 7.2 $7,955 $17,172 $4,144
$7,727 $8,410 $2,294 $3,785 $228 $2,522 $4,012
Self Pay 1 8.0 $0 $30,239 $6,269 $13,608 $3,441 $649 $1,548 -$13,608 -$12,959 -$12,059
All 425 7.4 $8,894 $26,820 $5,745 $12,069 $4,296 $1,052 $1,933 -$3,175 -$2,123
-$1,242
*Complete cost (including indirect costs) was estimated from the finding that inpatient cost averaged 45.0% of inpatient
charges.
Notes: Inpt denotes inpatient; LOS denotes length of stay.
Table A7. Financial analysis of medical respite per episode (St. Francis Hospital).
Hospital Annual
episode Before After
Change Reduction Hospital Payer Hospital Payer
Inpatient
episode
0.13 0.08
-0.05 0.60 $3,322 $6,215 $1,993
$3,729
Outpatient
episode
0.33 0.18 -0.15 1.80 $394 $325
$709 $585
Shorter hospitalization $1,933 $0
$3,060 $3,060 -$3,060 -$3,060
Total $1,575 $1,254
Monthly utilization per medical
respite recipient
Cost per episode
Annual savings to
stakeholder
Medical respite stay (50% each)

27
Sensitivity analyses
Figure A3 presents a sensitivity analysis exploring alternative divisions of the cost between the hospital
and the payer or funder (e.g., Medicaid) for St. Francis. The left axis corresponds to the scenario where
all of the cost of MR is covered by the payer or funder, and none by the hospital. As the share covered
by the hospital increases, the payer’s savings increase while the hospital’s savings decline. When the
hospital’s share crosses 30%, the payer achieves positive savings. However, once the hospital’s share
reaches 75%, the hospital’s savings drop to zero and then become negative.
Thus, if the costs of MR are divided so that the hospital’s share is between 30% to 75% of the costs (so
the payer’s share is 25% to 70%), then both parties realize financial savings from MR. At the
approximate midpoint (hospital and payer each fund 50% of the costs of MR), the hospital saves $1,575
while the payer gains $1,254 per MR admission.
Figure A4 summarizes St. Francis Hospital’s estimated savings per MR admission assuming the hospital
pays 50% of the cost of an MR stay. After paying this share, the hospital saves $1,575 per MR admission
through reduced losses from fewer subsequent inpatient admissions, a shorter index stay, and fewer
subsequent emergency room episodes. Assuming payers (such as Medicaid and other insurers) paid the

28
remaining 50% share of an MR stay, they would still save $1,254 per MR admission through their share
of savings from fewer subsequent inpatient admissions and emergency room episodes.
Figure A4
$1,993
$1,933
$709
-$3,060
$1,575
-$4,000
-$3,000
-$2,000
-$1,000
$0
$1,000
$2,000
$3,000
Savings per respite admission
St. Francis Hospital's estimated savings per medical respite
admission

29
APPENDIX 3: ADDITIONAL RESULTS FROM HOLY CROSS HOSPITAL
Table A8 shows the financial data of the 951 identified episodes of patients experiencing homelessness
by financial class for Holy Cross. Medicaid represents 25% of the charges. The absence of Medicaid
expansion in Florida limits eligibility, so a smaller share of patients experiencing homelessness were
covered by Medicaid than found in the case study in Connecticut, a Medicaid expansion state. Thus, the
hospital’s safety net was much larger, with charity and self-pay representing 27% and 6%, respectively,
of adjusted charges.
Explanation
Payments &
insurance
balance
Charges
% of
charges
Payments
as % of
charges
Charity
CHAR Charity $0 $2,944,594 27% 0.0%
Medicaid
MCD
Medicaid $153,098 $1,550,943 14% 9.9%
MCDMNG Medicaid managed care $104,929
$1,097,591 10% 9.6%
MCDPEND
Medicaid pending $4,237 $54,357 1% 7.8%
Total Medicaid $262,264
$2,702,891 25% 9.7%
Medicare
MCR Medicare $437,122 $2,935,138 27% 14.9%
MCRMNG Mediaid managed care $180,815 $644,323 6% 28.1%
Total Medicare $617,937 $3,579,461 33% 17.3%
Self Pay
SP Self pay (not fixed fee) ($99) $679,344 6% 0.0%
SPFF Self-pay fixed fee $5,792 $21,293 0% 27.2%
Total Self pay $5,693 $700,637 6% 0.8%
Other
BC Blue Cross $60,694 $150,007 1% 40.5%
CH Champus
$348 $5,027 0% 6.9%
CO Commercial $33,079 $179,264 2% 18.5%
WC Worker's compensation $822 $1,435 0% 57.3%
U Unknown $0 $1 0% 0.0%
HM Health Maintenance Org. $346,515 $584,451 5% 59.3%
Total
Other $441,459
$920,184
8% 48.0%
0%
Grand total All $1,327,353 $10,847,767 100% 12.2%
Financial class
Table A8. Payments as a percent of charges for patients experiencing homelessness at Holy
Cross Hospital (n=951 episodes)
Potential downstream impacts on health systems costs
Hospitals incur a loss on each episode of care provided to a person experiencing homelessness because
the hospital’s net revenue is below its cost for these patients. This loss occurs even if that patient is
covered by Medicaid and the hospital receives the Medicaid reimbursement. Table A9 shows the data
for Holy Cross Hospital by type of episode. As Florida lacks Medicaid expansion, Medicaid payments
cover a smaller share of the costs at Holy Cross than at St. Francis. For inpatient episodes, expected
30
payments average 52% of complete costs at Holy Cross compared to 65% at St. Francis. We estimate
these costs to be around $7,421 per inpatient episode and $490 per emergency episode. To show the
scale of the burden at Holy Cross hospital we projected the cost and net loss for all episodes identified
by the capture-recapture analysis. We estimate that serving people experiencing homelessness costs the
hospital $4.8 million with a net loss of $2.7 million annually. Table A10 presents the capture-recapture
calculations by setting, Table A11 shows details of the impact of a 2-day reduction of length of stay, and
Table A12 the detailed financial impact of an MR stay.
Notes: Exp denotes expected; pmt denotes payment
Table A9. Financial data and projections at Holy Cross by type of episode
Type of
episode
Charges
Complete
cost
Expected
payment
Exp.
pmt. as
% of cost
Net loss (N)
Inpatient $56,849 $15,349
$7,928 52% $7,421 150
Emergency $2,200 $594 $104 18% $490 623
Observation
$5,367
$1,449
$413 29% $1,036
177
Inpatient $13,189,064 $3,561,047
$1,839,267 52% $1,721,780 232
Emergency $3,037,883 $820,228 $144,138 18% $676,091 1,381
Observation
$1,685,128 $454,985
$129,766
29% $325,219 314
Total $17,912,075 $4,836,260
$2,113,171 44% $2,723,089 1,927
*Complete costs are estimated at 27% of charges, based on inpatient data
Actual amounts per episode
Projected aggregates for all episodes from capture-recapture analysis

31
Homeless
diagnosis
*
No Yes Total
Number of
identified
encounters
Number of
projected
encounters
Expansion
factor from
identified
encounters
Expansion
factor
from code
17
Inpatient
No
Unknown 40 40
Yes
74 36 110
Total 74 76 150 150 232 1.5 3.1
Emergency
No
Unknown 455 455
Yes
105 63 168
Total 105 518 623 623 1,381 2.2 2.7
Observation
No
Unknown 136 136
Yes
21 21 42
Total 21 157 178 178 314 1.8 2.0
Total
No
Unknown 631 631
Yes
200 120 320
Total 200 751 951 951 1,927 2.0 2.6
* Notes: ICD9-V60 or ICD10-Z59.
Address sources Number %
Code 17 742 39%
Diagnosis code, excluding previously
209 11%
Subtotal: all identified patients 951 49%
Projected total 1,927 100%
Table A10. Application of 'capture-recapture' method to estimating number of
homeless patients, Holy Cross*
Registration (code 17)
Application of capture-recapture

32
Financial
Class
Eligible
inpt.
stays
Avg.
LOS
Net
Revenue
Charges
Revenue
as % of
charges
Complete
cost
Surplus
(loss)
complete
stay
On charges
On
complete
costs
Aggregate amounts
Charity
32 5.8 $0 $1,466,628 0.0% $414,545 ($414,545) $271,183 $91,766
Medicaid
25 11.6 $211,300 $2,178,352 9.7% $700,362 ($489,062) $223,763 $87,213
Medicare
38 8.7 $523,053 $3,023,429 17.3% $718,341 ($195,288) $345,566 $109,640
Self Pay
14 4.9 $3,804 $475,462 0.8% $122,028 ($118,224) $104,852 $32,891
Other
8 8.3 $381,333 $794,444 48.0% $193,772 $187,561 $66,258 $21,809
All 117 11.9
$1,119,490
$7,938,315 14.1% $2,149,049 ($1,029,559) $1,011,621 $343,319
Average amount per inpatient episode
Charity 32 5.8 $0 $45,832 0.0% $12,955 ($12,955) $8,474 $2,868
Medicaid 25 11.6 $8,452 $87,134 9.7% $28,014 ($19,562) $8,951 $3,489
Medicare 38 8.7 $13,765 $79,564 17.3% $18,904 ($5,139) $9,094 $2,885
Self Pay 14 4.9 $272 $33,962 0.8% $8,716 ($8,445) $7,489 $2,349
Other 8 8.3 $47,667 $99,305 48.0% $24,222 $23,445 $8,282 $2,726
All 117 11.9 $9,568 $67,849 14.1% $18,368 ($8,800) $8,646 $2,934
Notes: Hospitalizations of fewer than 3 days were excluded. LOS denotes length of stay.
Table A11. Projected impact of a 2-day reduction in length of stay on a hospitalization of 3 or more days, Holy
Cross Hospital
Actual hospitalizations
Savings on 2-day reduct.
Table A12. Projected financial impact of one medical respite episode (MR, Holy Cross)
Annual
utilizatio
n per MR
Source of impact Before After
Change
Change
Hospital
Payer Hospital Payer
Fewer subsequent
inpatient episodes
0.13 0.08 -0.05 -0.60 $7,421 $7,928 $4,453 $4,757
Fewer subsequent
emergency
0.33 0.18 -0.15 -1.80 $490 $104 $881 $188
Subtotal $5,334 $4,945
2-day reduction in inpatient stay $2,934 $0
Subtotal savings on hospital utilization $8,268 $4,945
-$6,120
Total $8,268 -$1,175
Monthly utilization
per MR recipient
Loss per MR
episode
Annual savings
from MR episode
by stakeholder
Medical respite stay (payer funds all)
Notes: MR denotes medical respite.

33
Sensitivity analyses
Figure A5 presents a sensitivity analysis exploring alternative divisions of the cost between the hospital
and the payer or funder (e.g., Medicaid) for Holy Cross Hospital. The left axis corresponds to the
scenario where all of the cost of MR is covered by the payer or funder, and none by the hospital. As the
share covered by the hospital increases, the payer’s savings increase while the hospital’s savings decline.
When the hospital’s share crosses 19%, the payer achieves positive savings.
At the approximate midpoint (hospital and payer each fund 50% of the costs of MR), the hospital saves
$5,208 while the payer gains $1,885 per MR admission.

34
Figure A6 summarizes Holy Cross Hospital’s estimated savings per MR admission assuming the hospital
pays 50% of the cost of an MR stay. After paying this share of the cost of MR, the hospital saves $5,208
per MR admission through reduced losses from fewer subsequent inpatient admissions, a shorter index
stay, and fewer subsequent emergency room episodes. Assuming payers (such as Medicaid and other
insurers) paid the remaining 50% share of an MR stay, they would still save $1,865 per MR admission
through their share of savings from fewer subsequent inpatient admissions and emergency room
episodes.
Figure A6

35
APPENDIX 4: ADDITIONAL RESULTS FROM COMPARISON
Figure A7 shows the maximum break-even contribution to MR from each stakeholder in each hospital
and the combined amount. This contribution represents the amount at which the financial costs would
just equal the financial benefits. The horizontal lines for the combined amounts show the full cost of
MR, while the separate payers show 50% of this cost. The fact that the maximum contribution exceeds
these lines shows that the two payers could afford to support an episode of MR and still gain financially.
Furthermore, if the cost were allocated with 50% to each stakeholder, each would gain more than it
spends.
Notes: MR denotes medical respite.

36
REFERENCES
1. Edgington S, Shepard DS, Zeng W, Tschampl CA, Shetler D, Leackfeldt G, Bailey E and Chancy D.
Medical respite care for people experiencing homelessness: a preliminary analysis. National Summit for
Health Care Innovation Awards, Round 2 June 8, 2016.
2. Edgington S, Fader HC, Ramsay R, Harnish C and Clark B. Medical respite funding and return on
investment: panel discussion. May 31, 2016.
3. Dawe C, Lewine N and Miesen M. Today's most attractive national ACO model is offered by . . .
CMS. Health Affairs Blog. 15 Apr 2016.
4. Williams M. Can we measure homelessness? A critical evaluation of ‘Capture–Recapture’.
Methodological Innovations Online. 2010;5:49-59.
5. Crombie P, Shetler D, Cunningham A, Ferry M and Bozzo J. Columbus House Medical Respite
Data Analysis Presentation. Paper presented at: Opening Doors-Connecticut, Health and Housing
Stability Workgroup; August 2016; Hartford, CT.
6. Salit SA, Kuhn EM, Hartz AJ, Vu JM and Mosso A. Hospitalization costs associated with
homelessness in New York City. N Engl J Med. 1998;338:1734-1740.
7. Hwang SW, Weaver J, Aubry T and Hoch JS. Hospital costs and length of stay among homeless
patients admitted to medical, surgical, and psychiatric services. Med Care. 2011;19:350-354.
8. Feigal J, Park B, Bramante C, Nordgaard C, Menk J and Song J. Homelessness and discharge
delays from an urban safety net hospital. Public Health. 2014;128:1033–1035.
9. D’amore J, Hung O, W C and Goldfrank L. The epidemiology of the homeless population and its
impact on an urban emergency department. Acad Emerg Med. 2001;8:1051-1055.
10. Gallagher TC, Andersen RM, Koegel P and Gelberg L. Determinants of regular source of care
among homeless adults in Los Angeles. Med Care. 1997;35:814-830.
11. Kushel MB, Vittinghoff E and Haas JS. Factors associated with the health care utilization of
homeless persons. JAMA. 2001;285:200-206.
12. Zerger S. An Evaluation of the Respite Pilot Initiative 2006.
13. Zerger S, Doblin B and Thompson L. Medical respite care for homeless people: A growing
national phenomenon. J Health Care Poor Underserved. 2009;20:36-41.
14. Sadowski LS, Kee RA, VanderWeele TJ and Buchanan D. Effect of a housing and case
management program on emergency department visits and hospitalizations among chronically ill
homeless adults: a randomized trial. JAMA. 2009;301:1771-8.
15. Kertesz SG, Posner MA, O’Connell JJ, Swain S, Mullins AN, Shwartz M and AS A. Post-hospital
medical respite care and hospital Readmission of homeless persons. J Prev Interv Community.
2009;37:129-142.
16. Basu A, Kee R, Buchanan D and Sadowski LS. Comparative cost analysis of housing and case
management program for chronically ill homeless adults compared to usual care. Health Serv Res.
2012;47:523–543.
17. Shepard DS, Hodgkin D and Anthony YE. Analysis of Hospital Costs: A Manual for Managers.
2000.
